Below is the full, searchable text of the whistle blower complaint submitted by Dr. Richard ‘Rick’ Bright against the Department of Health and Human Services (DHHS) in its handling of the COVID-19 Coronavirus epidemic, its pushing of hydroxychloroquine, and its ouster of Bright himself.
The Internet Patrol makes no judgement nor offers any opinion about the contents of this whistleblower complaint by Dr. Rick Bright. The Internet Patrol is simply making it available because we know how, and people are searching for it.
Note that we are publishing this raw, so people can find it, and will be working throughout the day to format it.
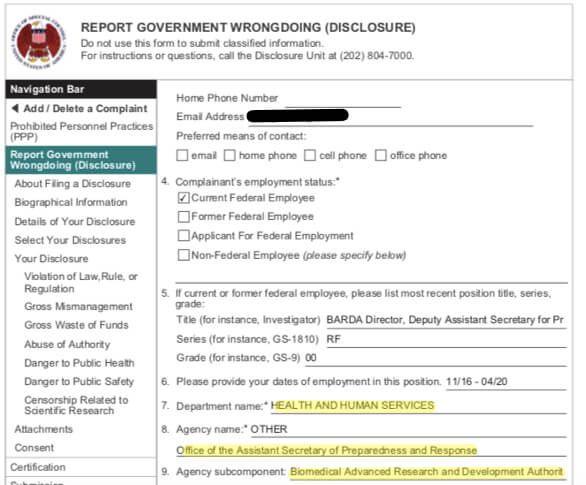
Also note that the below, while titled “Addenum to the Complaint of Prohibited Personnel Practice and Other Prohibited Activity by the Department of Health and Human Services Submitted by Dr. Rick Bright”, it is the meat of the complaint. It is the narrative attached to the standard form OSC-Form 14 used to report Prohibited Personnel Practices. A link to the PDF of the entire complaint, including the OSC-Form 14, is at the bottom of this article.
Also note that Dr. Bright is represented by the law firm of Katz, Marshall, and Banks, on whose letterhead the addendum to the complaint was submitted.
The Internet Patrol is completely free, and reader-supported. Your tips via CashApp, Venmo, or Paypal are appreciated! Receipts will come from ISIPP.
CashApp us

Venmo us

Paypal us

Addenum to the Complaint of Prohibited Personnel Practice and Other Prohibited Activity by the Department of Health and Human Services Submitted by Dr. Rick Bright
I. Introduction
Dr. Rick Bright is an internationally recognized expert in the fields of immunology, therapeutic intervention, vaccine, and diagnostic development. He is also one of the nations leading experts in pandemic preparedness and response and in the design of diagnostic tools required to track pandemics, such as COVID-19, a virus that at this writing has infected more than a million people in the United States and has already killed 70,000 people in our country alone.
Dr. Bright earned his PhD in Immunology and Molecular Pathogenesis (Virology) from Emory University, and has 25 years of experience working in government, industry, and nonprofit settings to research and develop drugs and vaccines responsive to emerging infectious diseases and to expand vaccine production capacity in the United States and around the world. He began his career researching viruses, immunology, vaccine development, and antiviral drugs at the Centers for Disease Control and Prevention (CDC), then transitioned into the biotechnology industry to oversee vaccine and immunology programs as the Director of Immunology at Altea Therapeutics. In 2003, the CDC recruited Dr. Bright to return and he worked to evaluate the comparative merits of antiviral drugs and developed rapid tests for antiviral drug resistance to help combat avian flu. In recognition of his exemplary work, the CDC awarded Dr. Bright the Charles C. Shepard Science Award for Scientific Excellence the most prestigious scientific award CDC confers. In 2006, Dr. Bright returned to the private sector as Vice President of Research and Development and Global Influenza Programs at Novavax, Inc., overseeing the development of new vaccines. In 2008, he joined the international health nonprofit PATH as the Scientific Director of the Influenza Vaccine Project in the Vaccine Development Global Program and the Director of the Influenza Vaccine Capacity Building Project in Vietnam, where he led efforts to accelerate the development and production of vaccines in developing countries.
In 2010, Dr. Bright joined the Department of Health and Human Services (HHS) as a Program Lead within the Biomedical Advanced Research and Development Authority (BARDA) Influenza Division International Program. In this role, he was responsible for expanding pandemic preparedness capacity to 12 developing countries, providing each with tools and capabilities to respond to a pandemic. In these countries, he led the expansion of vaccine production capacity from less than 1 million doses to a nearly 1 billion dose capacity during his tenure. In 2014, Dr. Bright became the Director of BARDAs Influenza and Emerging Diseases Division. In this role, he was responsible for preparing the nation for influenza pandemics and coordinating production, acquisition, and delivery of medical countermeasures during a pandemic response. In November 2016, after HHS completed a global competitive selection process, Dr. Bright was appointed Deputy Assistant Secretary for Preparedness and Response and Director of BARDA. Since 2008, Dr. Bright has also served in scientific advisory roles for the U.S. Department of Defense and the World Health Organization (WHO), working to advance vaccines and public health around the world.
Throughout his tenure as BARDA Director, Dr. Bright provided much needed leadership to this critical government agency and helped turn around an office that previously had high turnover and morale problems. Dr. Bright transformed BARDA into a larger, more stable, and better funded organization, hyper-focused on the single mission of developing drugs and vaccines to save lives. Dr. Bright worked tirelessly to lead a highly skilled technical team of government and industry partners in this mission. His efforts and successes were recognized and reflected in performance appraisals in which he was consistently given the highest possible ratings. See Bright Performance Evaluations, attached hereto as Exhibit 1. Dr. Bright and his team responded to the Zika and Ebola outbreaks and developed diagnostic tests, therapeutics, and vaccines that are being used today. When COVID-19 emerged as a global threat, Dr. Bright was uniquely positioned to lead BARDA in its crucial work of combating this existential public health threat. However, Dr. Bright repeatedly clashed with his supervisor Dr. Robert Kadlec, Assistant Secretary for Preparedness and Response (ASPR), who took orders from HHS Secretary Alex Azar. Their relationship had been tense since approximately 2018, when Dr. Bright began raising repeated objections to the outsized role Dr. Kadlec allowed industry consultants to play in securing contracts that Dr. Bright and other scientists and subject matter experts determined were not meritorious. Once the COVID-19 pandemic hit, however, Dr. Bright became even more alarmed about the pressure that Dr. Kadlec and other government officials were exerting on BARDA to invest in drugs, vaccines, and other technologies without proper scientific vetting or that lacked scientific merit. Dr. Bright objected to these efforts and made clear that BARDA would only invest the billions of dollars allocated by Congress to address the COVID-19 pandemic in safe and scientifically vetted solutions and it would not succumb to the pressure of politics or cronyism.
As detailed below, despite Dr. Brights efforts to ensure that the U.S. government dedicated the appropriate resources and expert personnel to combat this deadly virus, HHS political leadership leveled baseless criticisms against him for his proactive efforts to invest early in vaccine development as well as in critical supplies such as masks, respirators, and swabs, which were in short supply and would be necessary to combat COVID-19. Thereafter, HHS political leadership retaliated against Dr. Bright for his objections and resistance to funding potentially dangerous drugs promoted by those with political connections and by the Administration itself. Specifically, as detailed in the attached emails and other documentary evidence, Dr. Bright opposed the broad use of chloroquine and hydroxychloroquine as lacking scientific merit, even though the Administration promoted it as a panacea and demanded that New York and New Jersey be flooded with these drugs, which were imported from factories in Pakistan and India that had not been inspected by the FDA.
Dr. Bright felt an urgent and compelling need to inform the American public that there was insufficient scientific data to support the use of these drugs for COVID-19 patients particularly given their importation from factories abroad that had not been inspected by the FDA. Dr. Bright believed that Americans needed to have this critical information available to them to better inform them of the risks before taking the medicine. He also felt that he had exhausted all avenues to alert government officials, who refused to listen or take appropriate action to accurately inform the public. He concluded that his only remaining avenue was to share his concerns with a journalist who had contacted him and understood the specific issue and risks associated with these drugs and who had already gathered substantial information from multiple sources. Accordingly, Dr. Bright confirmed information for the reporter and provided corroborating documentation. He knew that providing this information to the reporter would place him at odds with HHS leadership. However as the death toll mounted exponentially each day, Dr. Bright concluded that he had a moral obligation to the American public, including those vulnerable as a result of illness from COVID- 19, to protect it from drugs which he believed constituted a substantial and specific danger to public health and safety.
Dr. Bright provided the reporter with emails between HHS officials that were not privileged or classified or otherwise legally restricted from dissemination, which discussed the drugs potential toxicity and demonstrated the political pressure to rush these drugs from Pakistan and India to American households. Dr. Bright hoped that by shining a light on HHSs reckless and dangerous push to make these drug available, American lives would be saved. HHS leadership, including Secretary Azar and Dr. Kadlec, were already gunning for Dr. Brights removal because of other issues he had raised about fraud, waste, and abuse, but they chose to remove him as BARDA Director within days of publication of the article about chloroquine because they suspected that he was the source. Coincidentally, on the very day that they involuntarily removed Dr. Bright from his position, the U.S. Food and Drug Administration (FDA) issued a warning that hydroxychloroquine and chloroquine have not been shown to be safe and effective for treating or preventing COVID-19.
Dr. Bright was removed as BARDA Director and Deputy Assistant Secretary for Preparedness and Response in the midst of the deadly COVID-19 pandemic because his efforts to prioritize science and safety over political expediency and to expose practices that posed a substantial risk to public health and safety, especially as it applied to chloroquine and hydroxychloroquine, rankled those in the Administration who wished to continue to push this false narrative. Similarly, Dr. Bright clearly earned the enmity of HHS leadership when his communications with members of Congress, certain White House officials, and the press all of whom were, like him, intent on identifying concrete measures to combat this deadly virus revealed the lax and dismissive attitude HHS leadership exhibited in the face of the deadly threat confronting our country. After first insisting that Dr. Bright was being transferred to the National Institutes of Health (NIH) because he was a victim of his own success, HHS leadership soon changed its tune and unleashed a baseless smear campaign against him, leveling demonstrably false allegations about his performance in an attempt to justify what was clearly a retaliatory demotion.
Here, the documentary evidence makes clear that Dr. Brights removal as BARDA Director was in retaliation for his whistleblowing activity under 5 U.S.C. 2302(b)(8)(A), which protects employees who disclose information that reveals any violation of any law, rule, or regulation, or gross mismanagement, a gross waste of funds, an abuse of authority, or a substantial and specific danger to public health or safety.
Because there are reasonable grounds to believe that Dr. Brights involuntary transfer to NIH constitutes a prohibited personnel practice, in violation of 5 U.S.C. 1214, the Office of Special Counsel (OSC) should request that HHS Secretary Azar stay this personnel action until OSC completes its investigation of Dr. Brights allegations. See 5 U.S.C. 1214(b)(1)(A)(i); Acting Special Counsel ex rel. Finkel v. Dep’t of Labor, 93 M.S.P.R. 409, 412 (2003) (hearing OSCs request for stay with MSPB upon the expiration of informal stay agreed upon by OSC and federal agency). Securing a stay of Dr. Brights reassignment will ensure that during the pendency of the OSC investigation, he will be able to continue to lead BARDA as the agency does its critically important work of partnering with industry to develop life-saving drugs and vaccines and combating the COVID-19 pandemic.
II. Since 2017, Dr. Bright Has Objected to HHS Leaderships Cronyism and Award of Contracts to Companies with Political Connections to the Administration.
BARDA, which is part of the HHS Office of the Assistant Secretary for Preparedness and Response (ASPR), was established in 2006 to assist in protecting the nation from bioterrorism, pandemic influenza, and emerging infectious diseases. BARDA supports the development and procurement of medical countermeasures against an array of threats to national security and the public health and acquires medical countermeasures (MCMs) in late stage development for the Strategic National Stockpile (SNS), the United States national repository of antibiotics, vaccines, and other critical medical supplies. BARDA oversees and executes government contracts and acquisitions with a cumulative value approaching $50 billion, and its average annual budget exceeds $1.5 billion.
BARDA achieves its mission by partnering with private industry. It provides funding, technical assistance, and services, including clinical research and manufacturing support, to facilitate and accelerate the research and development of essential drugs, vaccines, and diagnostics. A company that contracts with BARDA receives not only money, but also a wealth of expertise. BARDAs subject matter experts work with industry partners to troubleshoot issues, identify and mitigate risks, and achieve FDA approval. BARDA works primarily with drugs and technologies that have completed Phase 1 clinical trials and passed basic safety testing. While NIH generally supports companies through Phase 1 clinical trials, BARDAs funding and expertise bridge the valley of death between Phase 1 clinical trials and FDA approval.(1) BARDA has a unique and impressive track record, as 54 BARDA-supported products to date have achieved FDA approval and are either in the SNS or in the marketplace.(2)
— Footnotes —
1. In exceptional situations, including during the ongoing t(sic) COVID-19 health crisis, BARDA has flexibility to work with NIH to support drugs and technology that have not yet completed Phase 1 clinical trials. BARDA can give small awards and/or clinical expertise to companies working on compelling solutions that NIH lacks the capacity to support.
2. When BARDA was created, it was expected that, given the difficulty of achieving FDA approval, it would be able to secure approval for one drug every year or so. That BARDA has more than quadrupled that rate over the past 13 years demonstrates that its unique model is wildly successful. The combination of funding, in-house subject matter expertise, and industry expertise has resulted in a powerful virtual biotech company that has broken the mold for developing drugs and vaccines to support national security and biodefense medical countermeasures.
— End Footnotes —
Pursuant to BARDA Standard Operating Procedures, the agency solicits proposals by posting either a Request for Proposals (RFP), which seeks a specific kind of product, or a Broad Agency Announcement (BAA), an open-ended call for more innovative solutions. A BARDA contract officer (CO) reviews proposals submitted in response to an RFP or white papers submitted in response to a BAA, and passes along to a contract officer representative (COR) those submissions that comply with the relevant solicitation requirements. The COR then assembles a Technical Evaluation Panel (TEP) to review the submissions. TEPs generally consist of the reviewing CO and COR, as well as subject matter experts from BARDA, NIH, CDC, FDA, and the Department of Defense (DOD). TEPs review submissions and evaluate them based solely on scientific merit. They also rank the proposals submitted in response to an RFP. TEPs may request that companies provide additional information, or that authors of white papers submit formal proposals.
Importantly, BARDA may not consider the financial and business components of a proposal until after the TEP determines that the proposal has scientific merit. If a TEP recommends that BARDA accept a proposal, then a separate group consisting of some members of the TEP and others with budgetary experience reviews the budgetary aspects of the proposal and performs an Independent Government Cost Estimate (IGCE). The CO and COR then negotiate the budget and the final details of the work plan with the partner company and, if negotiations are successful, the COR and CO brief the Source Selection Authority (SSA), an individual who is authorized to approve the final contract.
Dr. Bright occasionally served as SSA but typically, and for all COVID-19 related proposals, the SSA was either Deputy Assistant Secretary and Director of Medical Countermeasures Programs Dr. Gary Disbrow, who reported to Dr. Bright, or Director of Influenza and Emerging Infectious Diseases Division Dr. Robert Johnson, who reported to Dr. Disbrow. Generally, Dr. Bright first became involved with a potential contract award after the SSA had decided to award a contract.
After a contract was approved, Dr. Bright was briefed on it and would often seek additional information on the relevant data, budget, challenges, timelines, and next steps. Dr. Bright was aware of every contract awarded by BARDA, but he did not have the authority, nor did he seek the authority, to award contracts and disperse BARDA funds unilaterally. Every contract is reviewed by a panel of scientific experts, typically from across HHS, and every contract passes through several layers of review before obtaining approval. Indeed, the review process is carefully monitored by various executives, as well as attorneys, in BARDA, ASPR and HHS. The focus of this rigorous review process is scientific merit, and the process is designed to allow no room for industry lobbyists, political influence, or special interests. Under Dr. Brights leadership as BARDA Director, contracts were to be awarded solely on the basis of scientific merit, best value for the governments money, and the potential to keep Americans healthy and safe.
After awarding a contract, BARDA works with the partner company to meet contract objectives and periodically holds an In-Process Review (IPR), chaired by the SSA, to assess the companys progress on milestones contained in the contract. During an IPR, the company makes a 30-60 minute presentation on its progress on the contract to a panel of interagency subject matter experts, often from BARDA, FDA, NIH, CDC, and DOD. The COR then briefs the same panel about his or her view of the companys progress and recommends whether, and the extent to which, BARDA should provide additional support to the company towards the next contractual milestone. If the company is struggling to achieve its stated goals, the COR may recommend decreasing the financial award, letting the contract expire or even termination of the contract. After the presentations and discussion, the IPR panel members are polled and the COR relays the panels recommendations to the SSA, who can approve or modify the IPR recommendation.
Despite this rigorous multi-level review process to ensure that BARDA prioritizes public health considerations and makes decisions based exclusively on scientific merit, from approximately the spring of 2017 through the date of his involuntary removal as Director of BARDA, HHS leadership pressured Dr. Bright and BARDA to ignore expert recommendations and instead to award lucrative contracts based on political connections and cronyism. Dr. Bright repeatedly clashed with Dr. Kadlec and other HHS leaders about the outsized role played by John Clerici, an industry consultant to pharmaceutical companies with a longstanding connection to Dr. Kadlec, in the award of government contracts.
As described in Section A, below, in the summer of 2017, Dr. Bright objected to the efforts of ASPR staff and Mr. Clerici to pressure Dr. Bright to extend a contract with Mr. Clericis client, Aeolus Pharmaceuticals (Aeolus), which an IPR had concluded should be allowed to expire without further funding. In attempting to justify the extension of this failed contract, Mr. Clerici emphasized that Aeoluss Chief Executive Officer was a wildcard and a friend of Jared Kushner, President Trumps son-in-law and a Senior Advisor to the President. Dr. Bright stood his ground on this contract, which led to some discord between him and HHS leadership. As discussed in Section B, below, Dr. Brights relationship with Dr. Kadlec and other HHS leaders became further strained in late 2018 after Dr. Bright objected to directions from Dr. Kadlec and his Chief of Staff, Christopher Meekins, to transfer $40 million from BARDA to the SNS to allow it to purchase generic Oseltamivir, a drug which a task force of experts had concluded was an inferior choice, in terms of scientific merit and public health preparedness, for the SNS compared to a competing drug developed and recently approved by the FDA. Dr. Kadlec ignored the objections of Dr. Bright and other experts and used BARDA funds to award a lucrative contract to purchase the inferior option, Oseltamivir, from the pharmaceutical company Alvogen, which was one of Mr. Clericis clients. As discussed in Section C, below, Dr. Bright also clashed with Dr. Kadlec and other members of HHS leadership when BARDA recommended awarding a task order on a contract only to Amgen to supply a drug for the SNS to treat radiation exposure rather than to both Amgen and Partner Therapeutics. Partner Therapeutics hired Mr. Clerici to manage its bid protest. Dr. Bright became so concerned about the improper role consultants such as Mr. Clerici played in promoting Partner Therapeuticss drug and their improper influence on Dr. Kadlec and HHS leaders that he requested that the HHS Office of General Counsel (OGC) initiate a procurement integrity violation investigation into the matter, and further that the OGC request an investigation by the Inspector General (IG) into outside influence on this contract. Dr. Bright subsequently learned that ASPR awarded a $55 million sole source contract to Partner Therapeutics, contrary to the original TEP decision.
As discussed in Section D, below, the pressure on Dr. Bright escalated in the fall of 2019, after he rejected pressure by Dr. Kadlec to invest millions of dollars in EIDD-2801, a drug developed at Emory University by a longtime friend of Dr. Kadlec. EIDD-2081 was presented as a miracle cure for influenza, Ebola and nearly every other virus, even though the developer had not yet conducted clinical trials and no data had been compiled to demonstrate either the efficacy or safety of the drug in humans. Dr. Brights reluctance to fund EIDD-2801, which had already receiving $30 million of government funding through NIH and DOD to conduct Phase 1 clinical trials, clearly frustrated Dr. Kadlec and further strained their relationship. Finally, as discussed in Section E below, Dr. Kadlecs frustration with and animus towards Dr. Bright reached its breaking point when, after the emergence of COVID-19, Dr. Bright resisted efforts to fall into line with the Administrations directive to promote the broad use of chloroquine and hydroxychloroquine and to award lucrative contracts for these and other drugs even though they lacked scientific merit and had not received prior scientific vetting. Dr. Brights refusal to do so, along with his communication with members of Congress, the White House, and the press about these issues, which revealed HHS leadership to be disengaged and dismissive of the emerging threat, proved to be Dr. Brights undoing.
A. ASPR Staff and John Clerici, an industry consultant and friend of Dr. Kadlec, exerted undue pressure on Dr. Bright to improperly extend a contract with Mr. Clericis client, Aeolus Pharmaceuticals.
In the spring of 2017, an In-Process Review (IPR) panel recommended that BARDA allow its contract with Aeolus Pharmaceuticals to expire. While Aeolus met initial milestones in its BARDA contract, it struggled to progress further. The IPR panel recommended that BARDA cease its financial support of the contract, and the SSA approved the recommendation. BARDA Chief of Chemical Medical Countermeasures (and contracts COR) Judy Laney, Acting Director of BARDAs Division of CBRN Medical Countermeasures Dr. Joe Larsen, Dr. Disbrow, and the contracts CO briefed Dr. Bright about the IPR recommendation, including that Aeolus was unhappy about the process. Because Dr. Bright greatly valued the integrity of the BARDA process and sought to ensure that process was fair to all involved, he directed the team to allow Aeolus to present all relevant data that the company felt was missing in the IPR. After allowing Aeolus to provide additional information, BARDAs determination did not change. BARDA informed Aeolus by letter that it would not exercise the additional options in the contract and it would expire. Aeolus immediately complained to media outlets that the BARDA process and decision was unfair.(3)
During July and August 2017, shortly after Dr. Kadlec became ASPR, Dr. Bright and his staff began receiving calls and emails from John Clerici, a pharmaceutical industry consultant who has longstanding connections with Dr. Kadlec, and who served on the Board of Aeolus.(4)
— Footnotes —
3. See, e.g., Aeolus Receives BARDA Decision Regarding Additional Options for Lung ARS Development Contract; Files Response to Assertions Made by BARDA in the Notification, MARKET INSIDER (Mar. 23, 2017), available at https://www.theinternetpatrol.com/brick-wall/ barda-decision-regarding-additional-options-for-lung-ars-development-contract-files-response-to- assertions-made-by-barda-in-the-notification-1001861859. See also Aeolus Receives BARDA Decision Regarding Additional Options for Lung ARS Development Contract; Files Response to Assertions Made by BARDA in the Notification, YAHOO! FINANCE (Mar. 23, 2017), available at https://finance.yahoo.com/news/aeolus-receives-barda-decision-regarding-120000495.html.
4. According to the website of Blank Rome, the law firm where Mr. Clerici is Of Counsel, Mr. Clerici has played a significant role in the creation and growth of the public health preparedness sector for nearly two decades, helping large pharmaceutical and emerging biotechnology companies access non- dilutive capital to fund the development of biotechnology for emerging disease and engineered threats. He has assisted more than three dozen companies in obtaining over four billion dollars in funding for the research …. See https://web.archive.org/web/20210730214004/https://www.blankrome.com/people/john-m-clerici. Mr. Clerici (along with Dr. Kadlec) was also pivotal in the drafting and passage of the Public Readiness and Emergency Preparedness Act, known as the PREP Act, landmark legislation that provides substantial protections against liability for makers and distributors of pandemic, epidemic, and bioterrorism countermeasures. Id. See also Coronavirus Has Created a New Golden Age for Vaccines, and Philly Is at the Heart of It, PHIL. INQUIRER (as reproduced by BLANKROME) (Apr. 3, 2020), available at https://web.archive.org/web/20210813235226/https://www.blankrome.com/news/coronavirus-has-created-new-golden-age-vaccines-and-philly-heart-it.
— End of Footnotes —
Consultants are often involved in the BARDA submission process by helping companies draft and submit proposals, but they are prohibited by federal law from engaging with BARDA officials after a proposal is submitted and before a contract is awarded.(5) While discussions between BARDA and its industry partners and representatives are not uncommon once a contract is in place, internal pressure from HHS leadership, such as the ASPR, to take actions to benefit certain individuals or companies is both unusual and improper. Once Dr. Kadlec came on board in August 2017, however, Dr. Bright and his team unfortunately began to experience such pressure.
On August 29, 2017, Mr. Clerici invited Dr. Bright to have coffee with him. During their meeting, Mr. Clerici clearly had the Aeolus contract in mind when he suggested that the BARDA review process was not always fair. He also remarked to Dr. Bright that some of these CEOs are high maintenance, and then referred specifically to Aeoluss CEO John McManus, with whom Dr. Bright was scheduled to meet with the next day. Mr. Clerici warned that McManus is a wildcard, and he is the kind of person who would write stories about you for the newspapers. Dr. Bright knew this to be true from the articles that had appeared the previous spring. Mr. Clerici also emphasized that Mr. McManus is friends with Jared [Kushner] and has Hollywood connections. Mr. Clerici, who has no formal scientific or medical training, then promoted the merits of a particular chemical in pharmaceutical drugs, which Dr. Bright suspected was related to the Aeolus contract. Dr. Bright became uncomfortable with the direction of Mr. Clericis comments and ended the meeting. Upon his return to the office, Dr. Bright confirmed that the specific chemical Mr. Clerici tried to promote over coffee was related to the Aeolus contract. It became clear to Dr. Bright that Mr. Clerici had been laying the groundwork for Mr. McManus to advocate that BARDA either revisit its prior decision about ending the Aeolus contract, or find a way for Aeolus to access the millions of unused contract dollars for a different project.
— Footnotes —
5. The Procurement Integrity Act (PIA), expressly bars consultants and lobbyists from participating in discussions regarding contract awards. See 41 U.S.C. 2101-07, implemented at Federal Acquisition Regulation (FAR) Part 3.104, 48 C.F.R. 3.104-3. Under the PIA, and the implementing FAR, a government official may not knowingly disclose contractor bid or proposal information or source selection information before the award of a Federal agency procurement contract to which the information relates. 41 U.S.C. 2102(a); 48 C.F.R. 3.104-3(a). On the industry side, a person shall not knowingly obtain contractor bid or proposal information or source selection information before the award of a Federal agency procurement contract to which the information relates. Id.
— End of Footnotes —
Dr. Bright met with Mr. McManus the next day, on August 30, 2017. Mr. McManus shared concerns that BARDAs decision about the Aeolus contract had not been arrived at fairly, including his specific concerns with the reasoning laid out in BARDAs letter informing Aeolus of its decision. Mr. McManus advocated for BARDA to reconsider its original decision or consider using the additional funds in the contract for another purpose. Dr. Bright explained to him that because the contract had been for specific data, the money could not simply be used for a different indication without submitting a new contract proposal. Dr. Bright also invited Mr. McManus to talk with the contracts SSA, Dr. Disbrow, about BARDAs decision because of Dr. Disbrows superior knowledge about the process on that decision. Instead of contacting Dr. Disbrow, however, Mr. McManus reached out directly to Dr. Kadlec to plead his case.
On September 27, 2017, Mr. McManus sent a letter to Dr. Kadlec requesting a meeting to discuss the Aeolus contract. That same day, ASPR Chief of Staff Christopher Meekins called Dr.Bright to discuss the Aeolus contract. Mr. Meekins informed Dr. Bright that Mr. McManus was making rounds on Capitol Hill because he was unhappy with where things stood with BARDA and asked Dr. Bright to prepare for a discussion on this issue with Dr. Kadlec. Mr. Meekins who, like Mr. Clerici, has no technical or scientific backgroundthen advocated the merits of the science behind the Aeolus contract. It became apparent to Dr. Bright that Mr. Clerici had been in touch with Dr. Kadlec and/or his staff, because Mr. Meekins made the very same points to Dr. Bright as Mr. Clerici had during their meeting over coffee.
On September 29, 2017, Mr. McManus met with Jennifer Alton, an HHS contractor working with Dr. Kadlec and who had previously worked with him in Senator Burrs office, to discuss the Aeolus contract. Three days later, on October 2, 2017, Mr. McManus sent an email to Ms. Alton thanking her for the meeting and reiterating the options they had discussed for a path forward with the existing or a new BARDA contract. Mr. Clerici was copied on the note, which Ms. Alton forwarded to Dr. Bright for discussion of those options. Dr. Kadlecs staff then asked Dr. Bright for a timeline to provide feedback on a proposed path forward. Dr. Bright informed Ms. Alton, as he had Mr. McManus during their meeting, that Mr. McManus would need to submit his information through the contracting office for proper proposal submission.
At this point, the political pressure from the new ASPR and his office became undeniable and was very concerning to Dr. Bright. Mr. Clerici, Dr. Kadlec, Ms. Alton, and Mr. Meekins were all well-connected, having worked with or for Republican members of Congress. Besides the fact that Mr. Clerici likely would profit from the contract, however, Dr. Bright did not understand why Mr. Clerici, Mr. Meekins, and Dr. Kadlec were united in a campaign to continue BARDA funding to Aeolus. Such pressure was clearly improper, and had no place in a system designed to award funding based on scientific merit and a determination of what projects were important to protect the public health. Dr. Bright insisted on merit and integrity, and he upheld the decision of the SSA to discontinue funding to Aeolus. Mr. Meekins on multiple occasions urged Dr. Bright to reconsider this decision, going so far as to suggest that BARDA find alternative uses for the drug Aeolus was producing. While Dr. Bright and BARDA stood by their decision and the improper pressure related to this contract ultimately failed, Mr. Clerici and ASPR staff continued to play an improper and outsized role in several BARDA contracts throughout the remainder of Dr. Brights tenure as Director.
B. Over Dr. Brights objections, ASPR ignored expert recommendations and used BARDA funds to award contracts to Alvogen, one of Mr. Clericis clients.
In late 2018, Dr. Kadlec and Mr. Meekins directed BARDA to set aside $40 million from BARDAs budget for the Strategic National Stockpile (SNS), the national repository of antibiotics, vaccines, and other critical medical supplies, to procure influenza antiviral drugs. During a meeting in the ASPRs office, Dr. Kadlec and Mr. Meekins instructed Dr. Bright to transfer $40 million to the SNS to purchase generic Oseltamivir, an influenza antiviral drug. Dr. Bright suggested that ASPR consider a different influenza antiviral drug, Xofluza, which was recently approved by the FDA. Subject matter experts had determined that it was critical to diversifying the SNS holdings, which would better prepare the SNS to save lives in a pandemic because viruses can become resistant to certain drugs. Indeed, a recent influenza virus had become resistant to Oseltamivir, the very drug the Dr. Kadlec and Mr. Meekins wanted to increase in the SNS. Dr. Bright urged Dr. Kadlec and Mr. Meekins to review the recommendations of subject matter experts, including Senior Advisor for Pandemic Medical Care and Countermeasures at the CDC Dr. Anita Patel, which supported his position. In an odd show of defiance, Mr. Meekins immediately began composing a text message to Dr. Greg Burel, the then-SNS Director, which he read aloud to Dr. Bright and Dr. Kadlec, about buying Oseltamivir instead of Xofluza.
Immediately following this meeting, Dr. Bright directed the interagency Flu Risk Management Meeting (FRMM) group to meet urgently to evaluate the SNS influenza antiviral drug holdings and recommendations. The FRMM is composed of influenza technical experts from within ASPR, BARDA, NIH, CDC, FDA, DOD, the United States Department of Agriculture (USDA), and the Department of Veterans Affairs (VA). It meets monthly to review influenza pandemic risk assessment data and to make recommendations to senior leaders about strategic preparedness investments in vaccines, drugs, diagnostics, and other essential medical supplies in the SNS. At Dr. Brights direction, the FRMM met in November 2018 to discuss recommendations for the SNS concerning the purchase of influenza antiviral drugs. On November 29, 2018, the FRMM issued a report calling on the SNS to prioritize the purchase of a newly- approved influenza drug called Baloxavir (Xofluza). The FRMMs official recommendation was for SNS to maintain Oseltamivir at the current inventory levels in the SNS meaning the SNS was not to purchase additional supplies of Oseltavmivir.
In December 2018, Dr. Bright, Dr. Johnson, and Director of the Influenza Division at the National Center for Immunization and Respiratory Diseases (NCIRD) at the CDC, Dr. Dan Jernigan, briefed the Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) executive leadership team, which Dr. Kadlec chairs, on the FRMM report. PHEMCE coordinates federal medical efforts to prepare the country for a potential public health emergency, such as from an emerging infectious disease. During the briefing, Dr. Bright, Dr. Johnson, and Dr. Jernigan presented FRMMs influenza antiviral recommendations and advised that the SNS accept those recommendations. The SNS was scheduled to brief the PHEMCE executive leadership team about its priorities at this same meeting, but that part of the meeting was postponed for reasons that were never explained to Dr. Bright.
Under the standard process, the SNS should have solicited the procurement of influenza drugs in accordance with the interagency FRMM recommendation. However, ASPR leadership was pressuring the SNS to procure additional Oseltamivir, instead of Baloxavir (Xofluza), in contravention of the express recommendation of the FRMM. Directed by Dr. Burel, the SNS ignored the interagency recommendation and instead began its own process to procure influenza drugs, deliberately excluding key influenza experts from BARDA and CDC as it wrote its own RFP. While the SNS has the authority to administer its own selection process, it was unusual for it to do so without the input of influenza experts, and against the express recommendation of the FRMM.
Dr. Bright believed that the FRMMs recommendation was best for public health and pandemic preparedness, and he was concerned about the undue influence that had been exerted on the SNS to deviate from the standard process. After looking into the matter, Dr. Bright learned that the SNS was planning to buy generic Oseltamivir from the pharmaceutical company Alvogen. Soon afterwards, Dr. Bright learned that Mr. Clerici was representing Alvogen and had been talking to Dr. Burel, Mr. Meekins, and possibly Dr. Kadlec about procuring Oseltamivir from Alvogen for the SNS.(6)
During an offsite pandemic preparedness exercise at George Mason University on January 23, 2019, Dr. Bright and Dr. Kadlec were having a conversation in the hallway when Mr. Clerici interrupted them to advise Dr. Kadlec that he was preparing Alvogen to submit a proposal for the SNS procurement of Oseltamivir. According to Mr. Clerici, he was confident he had Alvogen locked down for the purchase, i.e., that Alvogen was in line to get the award. Dr. Kadlec laughed uncomfortably and said something to the effect of, That sounds good to me. Im not sure I need to know all that right now. Dr. Bright remarked that he did not think more Oseltamivir was needed in the SNS. Again, Dr. Kadlec appeared uncomfortable and quickly changed the subject.
Following the meeting, ASPR and the SNS issued an RFP to procure influenza antiviral medicines and crafted the language in a manner that limited the types of drugs that could be considered for purchase, and seemingly to advantage Oseltamivir. In writing the RFP, ASPR did not consult with the influenza experts on the FRMM who had made a recommendation for Xofluza. Although BARDA and CDC subject matter experts tried to track the procurement process, ASPR and SNS kept the process closely held within a small group. During the RFP process and following questions from industry partners, the RFP was edited slightly to broaden the scope. On September 30, 2019, ASPR awarded a $40 million contract to Alvogen for generic Oseltamivir for the SNS. ASPR transferred funds from BARDA to facilitate the purchase of this drug for the SNS. Dr. Bright objected to this transfer, emphasizing that BARDA was in critical need of this funding to support other influenza medical countermeasure development and pandemic preparedness. Dr. Kadlec, clearly frustrated with Dr. Bright, dismissed his objections and told him sternly that he had no choice in the matter.
— Footnotes —
6. Oseltamivir had recently gone generic, and Alvogen was one of three different companies that produced it.
— End of Footnotes —
C. ASPR overruled subject matter experts to award a lucrative contract to Partner Therapeutics, one of Mr. Clericis clients.
Prior to 2018, BARDA had contracts with Sanofi-Aventis (contract transferred to Partner Therapeutics in 2017) and Amgen for similar drugs to treat radiation exposure. In June 2018, BARDA sought to exercise its option to procure more of the drug(s) for the SNS inventory, and it invited both companies to submit proposals. A panel of subject matter experts that included BARDA and SNS staff reviewed the proposals and recommended that an award be made to Amgen, and not to Partner Therapeutics. BARDA notified Partner Therapeutics of the decision in September 2018. Thereafter, Partner Therapeutics filed a bid protest, which the Government Accountability Office (GAO) dismissed on October 25, 2018, determining that the process had been fair.
Partner Therapeutics had hired Mr. Clerici to represent the company through the bid protest. Throughout the protest and subsequent proceedings, Mr. Clerici was in regular communication with Dr. Kadlec and his Chiefs of Staff, Mr. Meekins and Bryan Shuy, advocating that BARDA reverse its decision and exercise its option with Partner Therapeutics. The improper influence then trickled down to BARDA, when Dr. Kadlec, Mr. Meekins, and Mr. Shuy repeated Mr. Clericis talking points in favor of Partner Therapeutics to Dr. Bright. On several occasions, Mr. Meekins, Mr. Shuy and Dr. Kadlec called Dr. Bright into the ASPR office to share their scientific opinions and to try to convince him that the Partner Therapeutics drug was superior to the Amgen drug. They represented that a purchase from Partner Therapeutics was critical, because the company was having financial difficulties, and that BARDA should consider strategies to support the company. In both December 2018 and January 2019, Mr. Clerici contacted Dr. Bright to promote the Partner Therapeutics drug and denigrate the Amgen drug. Dr. Bright observed that Mr. Clericis talking points mirrored what he heard from ASPR staff, suggesting that they had been talking and coordinating their efforts.
At Dr. Brights direction, in late 2018, the HHS Office of General Counsel (OGC) initiated a procurement integrity investigation about the Partner Therapeutics proposal. In late summer 2018, Dr. Bright had learned that a senior BARDA employee had left and gone to work as a consultant for Partner Therapeutics. BARDA staff had observed that the Partner Therapeutics proposal was suspiciously aligned with BARDAs internal considerations, consistent with the possibility that Partner Therapeutics had knowledge of BARDAs internal process. The OGC investigation exposed involvement between the departing employee and Mr. Clerici, who was also working on behalf of Partner Therapeutics. Dr. Bright and his deputy, Dr. Disbrow, attended meetings with OGC attorneys and other HHS officials to address the potential violation and the bid protest, and if necessary, to take corrective actions. In the course of the investigation, it became clear that the primary source of improper communication about BARDAs internal deliberations was Mr. Clerici, who had been in frequent contact with Dr. Kadlec, Mr. Shuy, and Mr. Meekins.
During these meetings, Dr. Bright was vocal about his concerns regarding the inappropriate and possibly illegal communications between Mr. Clerici, Dr. Kadlec, Mr. Shuy, and Mr. Meekins. He also suggested that investigators inspect their phone records to search for evidence of their communications throughout the protest process. Dr. Bright even called for an investigation by the Inspector General (IG) to help break up the cottage industry of marketing consultants and political influence into these contracts. He emphasized that taxpayer dollars should go to lifesaving medicines, not marketing consultants. Dr. Bright was assured that after the procurement integrity issue was resolved, an IG investigation would commence, although he has no reason to believe it did. Instead, following his call for an IG investigation into Mr. Clerici and Dr. Kadlecs activities, Dr. Bright was excluded from all subsequent meetings involving the procurement integrity investigation and the resolution of this complaint.
After the investigation process was complete, Dr. Bright learned that Dr. Kadlec decided to award a sole source contract to Partner Therapeutics on the basis of industrial mobilization i.e.,the urgent need to keep a company financially viable.(7) In September 2019, the ASPR awarded a contract to Partner Therapeutics for $55 million, overruling the TEPs recommendation not to exercise the option on its prior contract. Dr. Bright, Dr. Disbrow, and Deputy Director of Detection, Diagnostics and Devices Infrastructure Division Dr. Mary Homer, the COR on the Amgen and Partner Therapeutic contracts, all objected to the ASPRs decision, but understood that ASPR had the authority to make a final determination that bound BARDA. Additionally, ASPR instructed the SNS to buy the drug exclusively from Partner Therapeutics to prevent the company from becoming bankrupt.
Even though Dr. Bright was cut off from the investigation and its conclusion, he took action to decrease future procurement integrity violations within BARDA. Dr. Bright directed his other Deputy Director, Dr. Linda Lambert, to work with the OGC to create a mandatory, two-session training program on procurement integrity for all BARDA employees. Also at Dr. Brights direction, Dr. Lambert and OGC developed and implemented a BARDA-wide organizational conflict of interest program, to thoroughly vet every existing and future BARDA contractor for any potential conflict of interest, and to implement processes to vet and train any new contract employees.
The fact that Dr. Kadlec and his staff repeatedly made decisions to benefit those like Mr. Clerici and his clients, but which were not in the best interest of the health or safety of Americans, continued to be of tremendous concern to Dr. Bright. As he continued to voice his opposition to these decisions and try where he could to push back, his relationship with Dr. Kadlec and HHS leadership deteriorated and became more contentious.
D. Dr. Bright resisted pressure from ASPR to fund a drug touted by Mr. Clerici and his client that lacked scientific merit.
On November 1, 2019, Dr. Kadlec held a meeting with Dr. Bright, Dr. Disbrow, Mr. Clerici, ASPR Senior Science Advisor Dr. David (Chris) Hassell, and Dr. George Painter, Director of the Emory Institute for Drug Development and President and Chief Executive Officer of Drug Innovation Ventures at Emory (Emory). During the meeting, Dr. Painter and Mr. Clerici presented a drug, EIDD-2801, as a cure all for influenza, Ebola, and nearly every other virus. They requested that BARDA urgently invest millions of dollars into their miracle cure. Emorys presentation included limited data, and no data at all from human trials. Dr. Bright asked targeted questions to understand the science behind the drug and its potential to safely treat patients. Dr. Bright knew that similar experimental drugs in this class had been shown to cause reproductive toxicity in animals, and offspring from treated animals had been born without teeth and without parts of their skulls. Dr. Bright accordingly asked Dr. Painter and Mr. Clerici about clinical trials, including whether Emory had conducted a reproductive study for toxicity, which they had not.
— Footnotes —
7. As a general matter, it is important to have more than one company in the supply chain able to make a particular drug in case need increases significantly or one company goes out of business. In this case, no such concern actually existed, as there were already three companies that produced similar radiation drugs, and generic equivalence could come soon, which would result in additional options.
— End of Footnotes —
Even before the presentation began, Dr. Kadlec indicated his enthusiasm for EIDD-2801s potential. Observing Dr. Brights skepticism during the presentation, Dr. Kadlec asked him why he was not similarly excited. Dr. Bright responded that he was excited about the potential of any promising new drug, but he knew that similar drugs produced fetal abnormalities, and his priority was to ensure drug safety. Unwilling to support a potentially toxic and harmful drug without further data, Dr. Bright asked when Emory planned to begin a clinical study. Dr. Painter and Mr. Clerici responded that Emory had already received $30 million in government funding from NIH and DOD to fund a clinical trial. Because Emory already had government money to fund toxicity studies and initial clinical trials, Dr. Bright suggested that Emory complete these studies and then, once it had amassed evidence that the drug was safe, return to BARDA to discuss funding. Dr. Bright noted that BARDA would then be able to make an informed decision based on scientific data. Dr. Painter countered that Emory needed BARDA funding to start manufacturing as soon as possible. He insisted that EIDD-2801 could be a great asset to American national security, and warned that if BARDA did not fund its manufacturing immediately, Emory would take the drug to another country to manufacture it. Dr. Bright asked where the drug was currently produced. Dr. Painter sheepishly admitted that it was made in China. Dr. Bright insisted that BARDA needed evidence that EIDD-2801was safe in humans before it could consider funding manufacture of the drug.
It was clear during the meeting that Dr. Kadlec was extremely unhappy with Dr. Brights reluctance to fund this drug immediately without further scientific study. Mr. Clerici, Dr. Painter, and Dr. Kadlec all advocated for immediate funding from BARDA, but Dr. Bright continued to insist on clinical testing, as was standard and proper procedure to ensure safety. Discussing the meeting afterwards, Dr. Disbrow remarked to Dr. Bright, Wow, you really pushed back. Nevertheless, following that meeting, Dr. Kadlec repeatedly called Dr. Disbrow and Dr. Bright to ask whether BARDA was going to support EIDD-2801. He also brought EIDD-2801 up in various staff meetings, asking Dr. Bright if BARDA had taken any steps to move forward with EIDD- 2801. Dr. Kadlec made it clear that he intended to push the funding through for this contract despite Dr. Brights objections.
To that end, in late 2019, Dr. Kadlec called for a meeting with BARDA, DOD, and NIH to discuss Emorys request for overall support of development of EIDD-2801. Dr. Bright had previously directed his staff to contact DOD and NIH to better understand the terms of their contracts with EIDD-2801, and at this group meeting convened by Dr. Kadlec, it was clearly stated that Emory had received sufficient funding through DOD and NIH to obtain the necessary data to inform further investment of government dollars. Dr. Bright again made it clear that he would not consider BARDA funding for EIDD-2801 until he had additional data from clinical trials.
Although Dr. Kadlec let it be known he was very unhappy with Dr. Brights position on this issue, the matter was tabled temporarily, as the country began to turn its attention to the emerging threat from COVID-19.
III. With the Emergence of COVID-19, Dr. Bright pushed BARDA to innovate quickly, but within the bounds of the scientific review process.
In late December 2019, Dr. Bright and other public health officials began taking note when a respiratory virus broke out in Wuhan, China. The CDC issued an official health advisory on January 8, 2020, and by January 11, 2020, the World Health Organization (WHO) had issued recommendations for countries to begin taking precautions to try to prevent the spread of COVID- 19. Given his decades of expert knowledge on pandemic influenza and emerging infectious diseases, Dr. Bright immediately understood the global reach of this virus. He recognized that lives would depend on the rapid development of effective diagnostics, treatments and vaccines and there was no time to waste. Dr. Bright acted with urgency to begin to address this pandemic but encountered resistance from HHS leadership, including Secretary Azar, who appeared intent on downplaying this catastrophic threat. According to an account in the Wall Street Journal, on January 29, 2020 eight days after the U.S. announced its first COVID-19 case Secretary Azar told President Trump that the coronavirus epidemic was under control and that the U.S. government had had never mounted a better interagency response to a crisis.(8) On February 27, 2020, Secretary Azar testified before the U.S. House of Representatives Ways and Means Committee that The immediate risk to the public remains low. He added, It will look and feel to the American people more like a severe flu season in terms of the interventions and approaches you will see.(9)
A. Dr. Bright encountered opposition from Administration officials as he began pressing for necessary resources to begin vaccine, drug, and diagnostic development.
Unlike Secretary Azar, Dr. Bright and other public health officials were fully aware of the emerging threat of COVID-19 by early January 2020. It was clear to Dr. Bright almost immediately that the virus was highly contagious, spreading rapidly, and could have a high mortality rate. Dr. Bright and his staff recognized the urgent need to obtain genetic sequencing information about the virus and to acquire viruses and clinical specimens from people infected with the virus to share with laboratories and companies. While obtaining both was absolutely critical to being able to develop reliable diagnostic tools and medicines to combat the virus, Dr. Bright initially encountered indifference which then developed into hostility from HHS leadership, including Secretary Azar, as Dr. Bright and his staff raised concerns about the virus and the urgent need to act.
— Footnotes —
8. Rebecca Ballhaus, Health Chiefs Early Missteps Set Back Coronavirus Response, WALL ST. J. (Apr. 22, 2020), available at https://www.theinternetpatrol.com/brick-wall/ coronavirus-response-11587570514.
9. Aaron Blake, 2 Months in the Dark: the Increasingly Damning Timeline of Trumps Coronavirus Response, WASH. POST (Apr. 21, 2020), available at https://www.theinternetpatrol.com/brick-wall/ increasingly-damning/.
— End of Footnotes —
On January 10, 2020, Dr. Bright received an update from Dr. Ruben Donis, BARDAs Deputy Director in the Influenza and Emerging Infectious Diseases Division, about the spread of the virus and he began pushing HHS leadership to obtain sequencing and virus samples from China, to no avail. In addition, Dr. Bright also began urgently pressing HHS officials to provide necessary resources to begin vaccine, drug and diagnostic development to combat COVID-19. Again, to no avail. Rather than deferring to Dr. Brights expertise and judgment and heeding his calls for urgent action, HHS leadership criticized him for his efforts and removed him from meetings going forward.
On January 12, 2020, the first novel coronavirus case was reported outside of China, in Thailand, raising levels of concern. The following day, the National Security Council set up a Policy Coordination Committee meeting for January 14, 2020, to discuss developments associated with the novel corona virus circulating around South East Asia. In response, Dr. Bright proposed an urgent agenda item for the meeting: We need to get virus samples to USG colleagues ASAP. Sequences alone are insufficient for potential mcm development and assessment…. For national security, we need more. See email from R. Bright to G. Disbrow (Jan. 13, 2020), attached hereto as Exhibit 2. Over the next several days, Dr. Bright met with ASPR and BARDA staff to discuss the outbreak and to review international reports regarding its spread. He repeatedly asked HHS Leadership to move quickly, hire more personnel, secure funding and obtain viruses to get started on medical countermeasures. His urgency was repeatedly met with seeming indifference by Dr. Kadlec who appeared to be focusing all of his attention and most of his ASPR resources on repatriating people from China and then from cruise ships with passengers infected by the Coronavirus.
On January 18, 2020, Dr. Bright pushed Dr. Kadlec and his ASPR policy group to coordinate senior level meetings, called Disaster Leadership Group (DLG) meetings, to coordinate planning activities across the government for the emerging COVID-19 outbreak. (In previous outbreaks, such as Ebola, Zika and influenza, the DLG played a central role in coordinating intergovernmental efforts to align on basic science and response activities.) Dr. Kadlec initially rejected Dr. Brights request to convene the DLG noting, Dont know if we HHS has (sic) outstanding policy issues to resolve. See email from R. Kadlec to R. Bright (Jan. 18, 2020), attached hereto as Exhibit 3. Later that day, Dr. Kadlec responded again, suggesting that while there was value to Dr. Brights suggestion to convene a DLG, he was [n]ot sure if that is a time sensitive urgency. Id. (Emphasis added.)
On January 20, 2020, the WHO held an emergency call, attended by many HHS officials, during which it advised that the outbreak is a big problem. After the call, Dr. Bright and his team discussed the need to make HHS leadership aware of the urgent necessity for funding to combat the virus. By email dated January 20, 2020, Dr. Robert Johnson, Director of BARDAs Division of Influenza and Emerging Infectious Diseases, asked Dr. Bright: Is the ASPR (and hopefully through him) the S1 [Secretary Azar] aware of just how BARDAs hands are tied due to lack of EID funding, and the precious time being lost? (emphasis in original.) See email from R. Johnson to R. Bright (Jan. 20, 2020), attached hereto as Exhibit 4. Dr. Bright responded that despite his request, Dr. Kadlec had still not held a DLG. Later that day, the first known case of coronavirus was reported in the United States, ratcheting up the sense of alarm that an outbreak in the United States was imminent. On January 21, 2020, Brian Shuy, Dr. Kadlecs Chief of Staff, emailed Dr. Bright and other BARDA officials requesting that they identify programmatic needs and estimate related costs. See email from B. Shuy to R. Bright (Jan. 21, 2020), attached hereto as Exhibit 5. Dr. Bright and his staff responded that virus samples and funds were urgently needed and, once again, Dr. Bright pushed Dr. Kadlecs staff to hold a DLG. Id.
At the same time that Dr. Bright was pushing HHS to obtain virus samples and increase funding to BARDA, he became convinced that as COVID-19 continued its rapid spread, the Administrations strategy of containing the virus (e.g., trying to prevent it from coming into the United States) was ill-conceived and that HHS needed to act urgently to increase supplies to be able to treat individuals who became infected when the virus began to spread in the United States. Dr. Bright was alarmed about the scarcity of critical resources and supplies, including N95 masks, swabs, and syringes, and began clashing with HHS leaders as he pressed for them to take appropriate action to address these shortages.
To the chagrin of HHS leaders, Dr. Bright repeatedly pushed Dr. Kadlec and the ASPRs critical infrastructure and supply chain teams to talk to mask producers and to secure and expand the U.S. mask supply. He also continually challenged them on the urgency of actions required to get in front of what he correctly identified as critical shortage issues.
On January 21, 2020, Mike Bowen, co-owner and Executive Vice President of domestic surgical mask producer Prestige Ameritech, emailed Dr. Bright to inform him that the Department of Homeland Security (DHS) had contacted him about procuring masks. See email from M. Bowen to R. Bright (Jan. 21, 2020), attached hereto as Exhibit 6. Dr. Bright forwarded the email to Dr. Kadlec, Mr. Shuy, Dr. Laura Wolf, Director of ASPR’s Division of Critical Infrastructure Protection (CIP), ASPR Director of External Affairs, Cicely Waters, and the SNS Deputy Director Steven Adams. Id. Dr. Bright asked Dr. Wolf to reach out to Mr. Bowen. In an email to Dr. Bright the following day, Mr. Bowen again offered to support the government in procuring masks. He explained that Prestige Ameritech had four N95 manufacturing lines that were currently not operational, but could be reactivated in a dire situation and with government help. He concluded the email by telling Dr. Bright, I hope that your and my predictions about the foreign made US mask supply dont come true. See email from M. Bowen to R. Bright (Jan. 22, 2020), attached hereto as Exhibit 7. Dr. Bright understood that the nation would need more masks, and Mr. Bowen offered a means of production from the countrys largest mask manufacturer. He responded that afternoon to thank Mr. Bowen for his offer. He explained that he had forwarded Mr. Bowens information to the ASPR critical infrastructure team the day before, and hoped that someone from the team had already contacted Mr. Bowen. In case they had not, Dr. Bright copied Dr. Wolf and Dr. Jessica Falcon, ASPR Deputy Assistant Secretary, on the email in hope of expediting a conversation. Id.
The next day, January 23, 2020, Dr. Kadlec finally convened a DLG meeting.(10) During the meeting, Dr. Bright emphasized BARDAs urgent need for virus samples and a major infusion of funds for development of diagnostics, drugs and vaccines. He also expressed concerns about the shortage of N95 masks, which he correctly anticipated would cause a health care crisis among first responders and health care providers. Disturbingly, Dr. Kadlec plowed through the abbreviated meeting, addressing topics in a perfunctory manner and paying short shrift to the concerns that Dr. Bright raised.
Also on January 23, 2020, Dr. Bright attended a meeting with HHS senior leadership across all agencies to brief Secretary Azar on COVID-19. Anticipating the urgency and magnitude of the threat and knowing the lead times needed to develop new drugs, diagnostics, and vaccines, Dr. Bright pressed for urgent access to funding, personnel, and clinical specimens, including viruses, which he emphasized were all critically necessary to begin development of lifesaving medicines needed in the likely event that the virus spread outside of Southeast Asia. Secretary Azar and Dr. Kadlec responded with surprise at Dr. Brights dire predictions and urgency, and asserted that the United States would be able to contain the virus and keep it out of the United States. Secretary Azar further indicated that the CDC would look at the issue of travel bans to keep the virus contained. Dr. Bright responded that virus might already be here. We just dont have the tests to know one way or the other. Dr. Brights comments were met with skepticism and were clearly not welcome. Nonetheless, he continued to press his point that the situation was dire and that money was urgently needed to develop diagnostics and drugs to combat the virus when it eventually spread to the United States. Secretary Azar then questioned Dr. Bright about BARDAs funding to combat the virus, to which Dr. Bright replied that BARDA had no funds available for emerging infectious diseases to meet the challenges of this pandemic, and that BARDA would be forced to re-direct funds from existing projects until new funding was made available. Secretary Azar also asked the representative from the Assistant Secretary for Financial Resources (ASFR) about availability of funding for the response.
It was evident from Secretary Azars reaction that this topic had not yet been raised at senior HHS levels.
Consistent with the attitude of Secretary Azar and Dr. Kadlec, HHSs public statements at the time likewise reflected no real sense of urgency. To the contrary, HHS publicly represented not only that COVID-19 was not an imminent threat, but also that HHS already had all the masks it would need. On January 23, 2020, an HHS spokesperson stated that CDC believes that the immediate risk to the U.S. public is low at this time. See Gretchen Michael, Media Key Points (Jan. 23, 2020), attached hereto as Exhibit 8. HHS also stated that the SNS holds millions of face masks as well as N95 respirators that could be used if needed in responding to a public health emergency when local supplies are exhausted and arent available from commercial suppliers.(11)
— Footnotes —
10. Apparently, the pressure and visibility of now having a case in the United States and Dr. Brights requests to hold a meeting to align across HHS and other government partners finally sank in and Dr. Kadlec scheduled a meeting with high level leaders from numerous offices and agencies.
11. See Jennifer A. Kingson, Coronavirus Fears Spark Run on Surgical Face Masks in U.S., AXIOS (Jan. 27, 2020), available at https://www.theinternetpatrol.com/brick-wall/ edf4-4d29-b24e-b10f16cbcd84.html.
— End of Footnotes —
As a result of the critical concerns raised by Dr. Bright in the January 23, 2020, meeting with Secretary Azar, HHS leadership excluded him from the next COVID-19 meeting, even though the agenda listed Dr. Bright as a participant. Mr. Shuy later told Dr. Bright that his request for urgent funding at the meeting on January 23th set off quite a shit storm after the meeting. Mr. Shuy further relayed to Dr. Bright he had offended HHS leadership by pushing for urgent funding, he had offended HHS leadership. According to Mr. Shuy, HHS leadership believed that BARDA already had a sizable budget, albeit nothing specifically for COVID-19, and that he should not have asked for additional resources to address the virus.
On January 23, 24 and 25, 2020, Mr. Bowen from Prestige Ameritech repeatedly emailed Dr. Bright and Dr. Wolf to sound the alarm yet again about the mask shortages. HHS failed to act yet again to address this impending emergency.
On January 25, Mr. Bowen wrote Dr. Bright and Dr. Wolf that his company was getting lots of requests from China and Hong Kong. He then explained that nearly 50% of masks in the United States are imported from Chinese manufacturers, and [i]f the supply stops, US hospital will run out of masks. No way to prevent it. See email from M. Bowen to R. Bright (Jan. 25, 2020), attached hereto as Exhibit 9. Dr. Bright forwarded Mr. Bowens email to the CIP Supply Chain, Dr. Wolf, Dr. Falco, and Mr. Adams, with a note that [t]he mask situation seems to be of concern and we have been receiving warnings for over a week. Id. Dr. Bright told the team that it was [i]mportant to keep this at the top of the heap of various issues. Id. As other countries were vying for the Unites States mask supply, Dr. Bright continued to put pressure on HHS leadership to take action, to no avail.
It became increasingly clear to Dr. Bright that HHS leadership was doing nothing to prepare for the imminent mask shortage, which Dr. Bright correctly recognized would hinder the ability of medical care providers and first responders to respond to this impending medical crisis. Accordingly, on that same day, January 25, 2020, Dr. Bright emailed Dr. Johnson and Dr. Disbrow about considering providing financial support to Prestige Ameritech to reopen its defunct factories. Dr. Johnson responded that he thought masks were within SNSs purview and budget. Nonetheless, Dr. Bright was skeptical that the SNS would move with the necessary urgency. That evening, Dr. Bright alerted Dr. Kadlec of the problem and encouraged him to accelerate a solution: Hearing face mask supply is also getting very low as China and HK trying to procure. Ive alerted cip on this throughout week. May need to consider options here also before things are gone. See email from R. Bright to B. Kadlec (Jan. 25, 2020), attached hereto as Exhibit 10.
The next morning, Mr. Bowen emailed Dr. Bright that the U.S. mask supply is at imminent risk. See email from M. Bowen to R. Bright (Jan. 26, 2020), attached hereto as Exhibit 11. Dr. Bright forwarded this dire warning to Dr. Kadlec, Dr. Wolf, Dr. Falcon, Dr. Disbrow, Dr. Johnson, Dr. Adams, and others, so they could see the basis for his alarm and insistence that action be taken at once. He wrote, We have been watching and receiving warnings on this for over a week. He then encouraged CIP and SNS to consider an action plan. Id. Dr. Bright wrote Mr. Bowen that stating: I know that our critical infrastructure protection team has been in contact with you. The next morning, Mr. Bowen responded, Ive spoken with Laura. Rick, I think were in deep shit. The world. Id.
Alarmed by HHSs inaction, on January 27, 2020, Dr. Bright emailed Dr. Disbrow to complain that Prestige Ameritechs requests for support to accelerate mask manufacturing seem[] (sic) to be falling on deaf ears. Understanding that HHS was not taking the necessary steps to prevent a mask shortage, Dr. Bright asked Dr. Disbrow whether BARDA should put in a budget request to assist.(12) Id. Later that day, Dr. Falcon emailed Dr. Bright to assure him that her office was having discussions about the mask concern. See email from J. Falcon to R. Bright (Jan. 27, 2020), attached hereto as Exhibit 12.
Also on January 27, 2020, Dr. Bright received an email from Dr. Larry Kerr, Director of Pandemics and Emerging Threats in HHS Office of Global Affairs, expressing an urgent need to talk about the CDCs failure to take appropriate actions to respond to the pandemic. See email from L. Kerr to R. Bright (Jan. 27, 2020), attached hereto as Exhibit 13. He stated: CDC just told the Secretary for his call with Minister Ma that [virus] samples from China are not needed and to de-prioritize it on the upcoming call. We fought back and I think he is still going to raise it but we need BARDA, NIH and FDA to speak up. The USG needs requirement is clear but CDC leadership is not saying that. Id. Dr. Bright replied that [w]e cannot emphasize enough the critical need to access virus to initiate MCM development. See email from R. Bright to L. Kerr (Jan. 27, 2020), attached hereto as Exhibit 14. Dr. Kerr responded that, as of that day, no one had officially asked China for samples. He further noted that Secretary Azar had had a call with Chinas Health Minister that morning but did not raise the need for virus samples.(13) Dr. Bright expressed disbelief at Secretary Azars failure to request virus samples, to which Dr. Kerr replied that Bob (Kadlec) was on the call but didnt speak up. Id.
That same morning, Dr. Bright participated in a COVID-19 meeting chaired by HHS Deputy Secretary Eric Hargan in Dr. Azars absence. During the meeting, Dr. Bright expressed frustration with the slow pace of accessing virus samples and/or clinical specimens from China, which he explained were critical to begin development of vaccines, diagnostics, and medicines. Dr. Bright asked pointedly why the CDC, which was securing viruses from other countries, was delaying providing them to BARDA or to companies to allow for MCM development. Dr. Nancy Messonnier, Director of the National Center for Immunization and Respiratory Diseases (NCIRD) at the CDC, who was participating by telephone, responded that Dr. Bright should know better than to make that request because he was well aware that the CDC had agreements with other countries that restricted it from sharing virus specimens with other entities, even within the government. Dr. Bright asked Dr. Messonnier to explain why these restrictions were in place and why BARDA could not use the material to get started on MCM development critical to save American lives. Dr. Messonnier became angry and chastised Dr. Bright, insisting that he take the topic offline.(14) Deputy Secretary Hargan, who was observing the conversation play out, gave Dr. Bright a hand signal to stop talking. It was clear to Dr. Bright that his inquiries had created tension.
— Footnotes —
12. In BARDAs initial budget formulation documents, a line item was included to expand domestic mask manufacturing lines. In the various internal discussions with ASPR, ASFR and BARDA, mostly lead by Mr. Shuy, BARDA was told to remove the budget request for mask production, that it purportedly was already covered in the ASPR and SNS budget line.
13. According to Dr. Kerr, in the pre-brief before Secretary Azars call with the Chinese Health Minister, it was emphatically expressed that BARDA, NIH, and FDA all disagreed with CDCs position and emphasized to Secretary Azar that there was an urgent need to secure a panel of viruses from China for MCM development.
14. Over the next few days, Dr. Bright and his team, at Dr. Brights direction, feverishly emailed health officials and laboratories in Australia, Thailand, the United Kingdom and France to try to obtain samples because the CDC had refused to provide information or virus samples to them. It was not even clear to Dr. Bright which virus samples, from the United States or other countries, the CDC actually had because the CDC refused to make this information available to other governmental agencies due its contractual obligations to the provider of the samples. Dr. Bright was alarmed by CDCs insistence that it adhere to contractual obligations that clearly impeded the governments ability to develop medical counter-measures to save lives.
— End of Footnotes —
The following day, Dr. Bright sent a note to Dr. Kerr to ask if the daily COVID-19 meetings with Secretary Azar were still occurring. Dr. Kerr confirmed that they were, but explained that due to the commotion in the meeting the day before, Judy Stecker, a high-level aide to Secretary Azar, decided that there were too many attendees and cut the list. Later that day, Dr. Bright sent an email to Dr. Kerr noting that he had heard that BARDA had been removed from briefings to Secretary Azar and asked if he had any insights. See email from R. Bright to L. Kerr (Jan. 28, 2020), attached hereto as Exhibit 15. Dr. Kerr responded that the decision to eliminate BARDA was made by Brian Harrison, Secretary Azars Chief of Staff, and Ms. Stecker, who decided that only Dr. Kadlec and his chief of staff, Mr. Shuy, who is not a scientist, would be permitted to attend and would present for BARDA. Id. It was obvious that Dr. Brights persistent demands for urgent action to respond to the pandemic had caused a shit storm and a commotion and were unwelcome in the office of the HHS Secretary. As a result, HHS leadership excluded Dr. Bright and BARDA from these recurring meetings and from the critical discussions about addressing the COVID-19 pandemic.
On January 29, 2020, Dr. Falcon sent another update to Dr. Kadlec, Dr. Bright, Mr. Shuy, and others regarding Identified Medical Supply Chain Focus Areas, which included N95 and surgical masks, and Concerns/Additional Analysis, which included the predominantly foreign production of masks. See email from J. Falcon to B. Shuy (Jan. 29, 2020), attached hereto as Exhibit 16. Dr. Falcons email did not list any action items, and despite weeks of warnings from Dr. Bright, industry leaders, and international media, her office was still not yet taking any action to procure masks. Two days later, Mr. Bowen of Prestige Ameritech sent yet another email to Dr. Bright and Dr. Wolf, once again issuing a dire warning about the imminent mask shortage. Id. Among other things, he advised [t]his week, we sent 1,000,000 masks to China and Hong Kong. He continued, [i]n all my years of predicting the US mask supply would one day collapse, I never pictured myself selling masks to China…. I have it from two reliable sources that China has begun telling Chinese mask makers not to let masks leave China. He concluded, I think China will cut off masks to the USA. If so, US hospitals are going to have a very rough time, as up to half of the supply is made in China. A horrible situation will become unbearable. See email from L. Wolf to R. Bright (Jan. 29, 2020), attached hereto as Exhibit 17. (emphasis added). Dr. Wolf followed up with Dr. Bright to let him know that CIP and CDC were working with N95 manufacturers and distributors. She told Dr. Bright that [t]here is cause for concern, but not panic. Id.
On February 3, 2020, Mr. Bowen sent yet another dire warning about the mask supply shortage and urged Drs. Bright and Wolf to speak to a New York Times reporter whom Bowen had contacted about this growing threat. He urged them to speak to the media to make the president aware of this little known national security risk. If we let this opportunity go by, the US mask supply will forever remain under foreign control. Trump reads the news. See email from M. Bowen to R. Bright (Feb. 3, 2020), attached hereto as Exhibit 18. Dr. Bright did not speak with the reporter, but instead followed the chain of command and referred the matter to HHSs communications team. By February 4, 2020, the media was reporting an impending global mask shortage.(15) Unfortunately, the public exposure of this aspect of the impending health crisis did not cause HHS leadership to act. That week, noting that no other office was taking appropriate action, Dr. Bright directed BARDA to revise its budget to include expenses to ramp up domestic mask production. However, in the following weeks of budget negotiation between BARDA, ASPR and ASFR, it was determined that the budget for masks would be covered under the ASPR SNS budget and removed from the BARDA budget request.
During late January/early February 2020, Dr. Bright also launched a comprehensive review of existing drugs that had been developed for MERS, SARS, Ebola and other viruses to urgently determine if there might already be a drug available or in late stage development that could work against the novel coronavirus. Dr. Bright had BARDA create a landscape chart that showed all possible vaccine, therapeutic and diagnostic candidates that might be efficacious in the treatment of the novel coronavirus. In addition, BARDA had made significant investments in various drug and vaccine platform technologies common backbones and production systems used to make vaccines and treatments for other viral threats that could be leveraged to move much faster to develop a treatment or vaccine for the novel coronavirus. Dr. Bright had his team chart and prioritize these platforms for rapid assessment of their potential for use in the outbreak. In addition, Dr. Bright directed his team to review all existing contracts and agreements to assess which agreements could be quickly refocused to address the novel coronavirus. This strategy had been put in place at BARDA over the last five years to respond quickly to emerging infectious diseases. Under Dr. Brights direction, BARDA was executing its long-standing strategic plan for rapid response to an emerging virus.
In conducting this assessment, Dr. Bright became concerned about the limited supply of Remdesivir, a broad-spectrum antiviral medication developed by Gilead Sciences (Gilead) that appeared, based on limited data coming from China and some laboratory-based testing, to lower the number of days it took patients to recover from COVID-19. After reviewing available scientific and medical literature, Dr. Bright and HHS and global clinicians determined that Remdesivir had the highest probability of an existing drug for being efficacious for treating people with COVID-19. He further determined that Gileads supply of the drug was low it had only a few thousand doses of the drug on hand and the timeline to manufacture more was lengthy. He repeatedly advised Dr. Kadlec and other HHS officials of the urgent need to acquire the existing doses and to secure future doses as they were produced. He also strongly recommended that HHS work with Gilead to on-shore all steps of the Remdesivir supply chain to ensure an uninterrupted supply in the United States. Once again, Dr. Brights urgent requests for concrete measures such as these only escalated tensions with HHS leadership, which apparently wished to downplay the risk of the virus and therefore intended to marginalize him and exclude him from key meetings as he continued to sound the alarm.
— Footnotes —
15. Maryn McKenna, Amid Coronavirus Fears, a Mask Shortage Could Spread Globally, WIRED (Feb. 4, 2020), available at https://www.theinternetpatrol.com/brick-wall/ spread-globally/ (quoting Mr. Bowen).
— End of Footnotes —
On February 7, 2020, the DLG met and, at Dr. Brights urging, focused on the topic of masks and respirators. Dr. Bright and Dr. Anita Patel from the CDC reminded DLG members of previous FRMM reviews, models and publications which cited a need for up to 3.5 billion N95 masks to respond to a pandemic. Dr. Bright reiterated that the United States had a significant shortage and raised concerns that the exportation of masks further depleted an already inadequate supply. He insisted that the federal government urgently needed to place orders to ramp up production of N95 masks in order to ensure that health care workers and first responders were adequately protected. This was crucial to ensure their own safety and also to prevent the spread of COVID-19 in hospitals and other medical settings. ASPR supply chain leads pushed back, insisting that there was no indication of a supply chain shortage or of issues with masks, and therefore there was no need to take immediate action. Dr. Bright responded that the country was already seeing shortages in drug stores and online and it was clear that there was going to be a dangerous shortage of masks as the virus continued to spread. Dr. Wolf and Dr. Falcon responded that the plan was to monitor for any supply chain issues and, if needed, ask the CDC to update its guidelines to tell people who don’t need masks to not buy them. Dr. Bright responded, I can’t believe that you can sit there and say that with a straight face. Do you really believe that changing a CDC guideline to tell people not to wear masks would reduce the panic people would feel once this virus spreads? He again emphasized the need to contact mask producers to place orders immediately.
Fortunately, White House Trade Advisor Peter Navarro shared Dr. Brights sense of urgency, recognized his expertise, and was prepared to help. Mr. Bowen, who continued to raise concerns about the dire consequences of the mask shortage in the United States, connected Mr. Navarro with Dr. Bright. On February 5, 2020, Mr. Bowen sent Dr. Bright an email marked High Importance, with the subject line: Prepare for a call from the White House. He stated: Im pretty sure that my mask supply message will be heard by President Trump this week. Im getting a ton of press and saying that youre the guy who knows that Im telling the truth. Thanks to a Trump insider reading yesterdays Wired.com article the ball is screaming toward your court. Im handing you the power to fix the US mask supply. Please dont let American (sic) down. See email from M. Bowen to R. Bright (Feb. 5, 2020), attached hereto as Exhibit 19. Mr. Bowen continued: Im also telling people that you [and the former director of BARDA] are exemplary public servants. I know that youre doing whats in your power… Please ask your associates to convey the gravity of this national security issue to the White House. Im pretty sure youll get the chance. Id. Dr. Bright again followed the chain of command and made the ASPR office was aware of Mr. Bowens entreaty that day by email. The following day, the Wall Street Journal ran an article about the mask shortage, once again sounding the alarm.(16) And once again, HHS Leadership failed to act.
— Footnotes —
16. See Austen Hufford, Coronavirus Outbreak Strains Global Medical-Mask Market, Wall St. J. (Feb. 6, 2020), available at https://www.theinternetpatrol.com/brick-wall/ mask-market-11580985003.
For that reason, on February 7, 2020, Dr. Bright was greatly surprised and relieved to receive a telephone call from Mr. Navarros policy assistant, Joanna Miller, who was with Mr. Navarro in the White House Situation Room. Ms. Miller asked Dr. Bright to meet with Mr. Navarro and members of his staff the following day at the White House to brief them about coronavirus response activities. Dr. Bright told Ms. Miller that he was eager to meet with Mr. Navarro but required the approval of HHS leadership to attend the meeting. He then immediately contacted Dr. Kadlec to obtain authorization to attend. Dr. Kadlec informed Dr. Bright that he (Kadlec) needed to discuss the request with Secretary Azar. As the meeting time approached, Dr. Kadlec had still not responded to Dr. Brights request to attend the meeting with Mr. Navarro. When Dr. Bright notified Mr. Navarro that he had not obtained clearance to attend the meeting, Mr. Navarro called both Dr. Kadlec and Brian Harrison, Secretary Azars Chief of Staff, directly. A few minutes later Dr. Kadlec emailed Dr. Bright, you (sic) cleared to attend. Thank you for advising. See email from R. Kadlec to R. Bright (Feb. 8, 2020), attached hereto as Exhibit 20. Even though Dr. Kadlec authorized Dr. Bright to attend the meeting, he was extremely uncomfortable that Dr. Bright had agreed to meet with Mr. Navarro. Dr. Bright later learned that Mr. Shuy had sent Ms. Miller two emails trying to dissuade Mr. Navarro from meeting with Dr. Bright. After Dr. Bright and Mr. Navarro met, Dr. Kadlec and other members of HHS leadership made disparaging remarks about Dr. Brights interactions with Mr. Navarro and the White House.
At 2:00 p.m. on Saturday, February 8, 2020, Dr. Bright met with Mr. Navarro at the White House. Dr. Bright found Mr. Navarro to be deeply engaged in the issues confronting the United States in responding to the rapidly approaching pandemic. Mr. Navarro clearly shared Dr. Brights concerns about the potential devastation the United States would face from the coronavirus and asked Dr. Bright to identify the supply chain and medical countermeasures most critical to address at that time in order to save lives. Dr. Bright emphasized the need to secure N95 masks and to ramp up mask production. He also informed Mr. Navarro about other actions that were urgently needed to develop diagnostic tools, drugs, and ultimately a vaccine, to combat the virus. In the short run, Dr. Bright urged Mr. Navarro to take immediate action to increase the mask supply, amass Remdesivir, and fund and initiate a Manhattan Project for vaccine development. Unlike Secretary Azar, Dr. Kadlec and other members of HHS leadership who dismissed Dr. Brights assessments and urgent requests and excluded Dr. Bright from key meetings, Mr. Navarro asked good questions and was prepared to take prompt action to address this impending health crisis. Mr. Navarro clearly recognized that Dr. Bright was unable to get any traction with HHS and was, to Dr. Brights great relief, prepared to act.
Indeed, the following day, Mr. Navarro invited Dr. Bright to return to the White House to assist him in preparing a memorandum to the White House Coronavirus Task Force urging it to direct HHS leadership to take three critical steps. In this memorandum, which Mr. Navarro sent through President Trumps Chief of Staff, Mick Mulvaney, and President Trumps National Security Advisor, Robert OBrien, he identified three actions to be undertaken IMMEDIATELY. See Memorandum to the Task Force, (Feb. 9, 2020), attached hereto as Exhibit 21. They were: 1) immediately halt the export of N95 masks and ramp up U.S. production of masks; 2) secure all existing doses of Remdesivir and all bulk materials to make more and enter into a contract with Gilead to purchase all additional doses as they are produced; and 3) immediately fund and initiate a “Manhattan Project” for vaccine development. In explaining the need for a Manhattan Project for vaccine development, Mr. Navarro stated in the memo:
There is currently no vaccine to protect against coronavirus. If we start this week to fast track vaccine development with appropriate funding, we can likely have a vaccine to clinical trials within 7 months and a workable vaccine by October or November, with a production capacity of 150 million doses by the end of the year IF we act NOW. We dont yet know what type of vaccine would be safe and effective. Therefore, it is critical the USG invest in multiple shots on goal to ensure that at least one vaccine is realized. Efforts should be prioritized to focus on US- based vaccine companies with extensive experience with being licensed by the FDA or with significant human safety data.
Mr. Navarro ended the memorandum stressing the importance of leaving the next task force meeting with a firm decision to immediately advance all three recommendations and warned that [i]naction at this point risks losing our Remdesivir drug supply, our N-95 production capabilities, and any head start we may have on a vaccine for next year. Id.(17)
The following day, Monday, February 10, the National Security Council Policy Coordination Committee met and directed Dr. Kadlec and HHS leadership to implement Mr. Navarros recommendations. This push by the White House for HHS to act more swiftly created tension between Dr. Bright and HHS political leadership because they knew that by meeting with Mr. Navarro, Dr. Bright had clearly played a key role in getting the White House Task Force to issue these directives. Dr. Kadlec in particular was uneasy about Dr. Brights time with Mr. Navarro, and he and other employees in Secretary Azars office kept tabs on their communications. That same day, Dr. Bright sent Dr. Kadlec a detailed email briefing him about the areas he had discussed with Mr. Navarro. See email from R. Bright to R. Kadlec (Feb. 10, 2020), attached hereto as Exhibit 22. While Dr. Kadlec blandly responded thanks Rick to that email, he sent another email to Mr. Harrison, Ms. Stecker, and Mr. Mango, copying Dr. Bright and Mr. Shuy, with a subject line Weekend at Peters that was a clear jab at Dr. Bright. In it, he suggested that it may be worthwhile to get a back brief from Rick Bright on his time with Navarro. See email from B. Kadlec to B. Harrison (Feb. 10, 2020), attached hereto as Exhibit 23. There was no follow up on this suggestion and no one at HHS asked Dr. Bright to provide them with a debriefing.
— Footnote —
17. Dr. Kadlec criticized Dr. Bright for his insistence that the U.S. start working on vaccines at the outset of the pandemic, stating that the focus should be on drugs because vaccines would take too long to develop. It took Secretary Azar until April 10, 2020, to focus on the need to prioritize vaccines and to come up with a Manhattan Project for vaccine development. Indeed, it was not until the period between April 13 to April 17, 2020, when Dr. Peter Marks, Director of the FDAs Center for Biologics Evaluation and Research, presented his Project Warp Speed project to Secretary Azar that he (Azar) embraced such an approach. By the time Secretary Azar and others in HHS Leadership focused their attention on vaccine development, BARDA, under Dr. Brights leadership, already had 40 contracts in place with companies to rapidly develop medical countermeasures for COVID-19, three of those were for vaccines with more contracts were in negotiation.
— End of Footnotes —
While Dr. Kadlec remained uncomfortable with Dr. Brights access to the White House, he was left with no choice but to implement actions that mirrored those set out in Mr. Navarros memorandum. At an ASPR Senior Leadership meeting on February 10, 2020, Dr. Kadlec announced an urgent directive to his staff that included, as its top three priorities: (1) stopping exports of masks and preparing for an increased demand for N95s; (2) buying all existing Remdesivir; and (3) managing vaccine candidates like a Manhattan Project. See email from L. Lambert to R. Bright (Feb. 12, 2020), attached hereto as Exhibit 24. Because of Dr. Brights meeting with Mr. Navarro, HHS had for the first time committed to taking certain actions to protect the countrys supply of masks, among other things.
Despite Dr. Brights best efforts, to connect mask producers to the ASPR supply chain leads so they could hear first-hand from manufacturers about the growing shortage, this urgent issue had not been effectively addressed. Accordingly, Dr. Bright continued to offer dire warnings and forward reports of mask shortages to the ASPRs SNS and Critical Infrastructure teams. But while more discussion was occurring, little action was taking place to address this significant risk. Indeed, on February 14, 2020, Dr. Kadlec and Mr. Shuy were asked to brief Mr. Navarro on medical supply chain issues and asked the ASPR supply chain leadership to prepare slides for the meeting. Shockingly, the conclusion was that there are no known immediate problems with supply chains even though there was an acknowledgement that the United States could require up to 6 billion respirators in a pandemic, and that it was [u]nlikely that the US will have enough disposable N95 respirators to meet response needs under current infection control recommendations. See COVID-19 (2019-nCoV): Medical Supply Chain (Feb. 14, 2020) (slide deck), attached hereto as Exhibit 25, at pages 3 and 4. Later in the report, ASPR identified other critical products of concern, including face shields, needles, syringes, and antimicrobials, and identified as important issues of concern a shortage of gloves and gowns. Id at pp. 12-13. Thus, even as HHS leadership began to acknowledge the imminent shortages in critical medical supplies, they failed to recognize the magnitude of the problem, and they failed to take the necessary urgent action.
Later in the day on February 14, Dr. Bright returned to the White House at Mr. Navarros request to assist him in drafting several more urgent memos in preparation for the Task Force that were necessary, in Mr. Navarros words, to get shit done and save lives. Dr. Bright briefed Mr. Navarro about the meeting referenced above and its conclusions, and like Dr. Bright, Mr. Navarro was extremely concerned about HHSs laxity in addressing the pandemic. He requested Dr. Brights assistance in drafting memoranda to the White House Task Force about production of N95 masks, respirators, vaccines, therapeutics, diagnostics and ancillary supplies such as needles and syringes that were critical to administer vaccine. In the course of this and other meetings, Dr. Bright briefed Mr. Navarro about the urgent need to develop rapid, hand-held diagnostic and serology tests and potential shortages of materials necessary to administer COVID-19 tests, such as swabs and extraction buffers. He made clear that the lack of masks and protective equipment put health care workers at serious risk and that without adequate masks and Personal Protective Equipment (PPE), they would be extremely vulnerable to infection. He also discussed with Mr. Navarro his growing alarm about the shortage of syringes, needles and vials necessary to administer vaccines if and when one became available.
At the conclusion of the February 14th meeting, Mr. Navarro drafted five separate memoranda to the White House Task Force, urging: the production of N95 masks; the creation of a Manhattan Project for the development of oral antiviral drugs; the mass production of manufacture of needles and syringes; the development of handheld diagnostic and serology tests; and the development of monoclonal antibodies for potential prophylactic use to protect healthcare workers and other critical workers until a vaccine became available.
Mr. Navarro sent three memoranda to the COVID-19 Task Force, through Mr. Mulvaney and Mr. OBrien, urging immediate action to increase production of Remdesivir, increase the N95 face mask supply, and ramp up production of needles and syringes necessary to deliver a vaccine. See Memo to Covid-19 Task Force: Ramp Up Production of Ancillary Supplies, (Feb. 14, 2020), attached hereto as Exhibit 26; Memo to Covid-19 Task Force: Expand Remdesivir Production to Include a US-Based Production Facility, (Feb. 14, 2020), attached hereto as Exhibit 27; Memo to Covid-19 Task Force: Status of N-95 Face Mask Supply, (Feb. 14, 2020), attached hereto as Exhibit 28. With respect to the ancillary supplies issue, Mr. Navarro stated:
We face an urgent need to administer large quantities of vaccine once produced. An estimated 850M needles and syringes are required to deliver vaccine. Our current inventory of these supplies is limited and, under current capabilities, it would take up to two years to produce this amount of specialized safety needles. We may find ourselves in a situation where we have enough vaccine but no way to deliver all of it.
Id. (Emphasis added.) Mr. Navarro made the following recommendations, all of which Dr. Bright had suggested:
Recommendations
Direct OSHA and CDC to take steps to liberalize the current policies to allow for the use of non-specialized needles to administer vaccines. Current delivery is with specialized needles with safety caps that have limited production capacity. This one change would significantly increase available inventory.
Provide HHS Strategic National Stockpile with immediate funding to place orders to ramp up US production to full capacity for needles and syringes needed to deliver a vaccine. We need to immediately determine budget needs and allocate accordingly.
Direct HHS BARDA to initiate a program to identify all alternate vaccine delivery methods and ramp up production. Other delivery possibilities include jet injectors and similar devices, some of which are already approved to deliver influenza vaccines.
Id.
On February 15, 2020, the Shortages Team within the FDA Center for Devices and Radiological Health, Office of Product Evaluation and Quality, emailed Prestige Ameritech President Dan Reese, requesting that he complete a five-page form about his companys ability to manufacture PPE for the national emergency response to COVID-19. Mr. Reese forwarded the request to Mr. Bowen, who responded to the FDA by criticizing the government for being so slow to act. Mr. Bowen was angry and frustrated that Prestige Ameritech had repeatedly warned the government about the imminent mask shortage, invited them to discuss with him ways to address the issue, and had received no response, other than a form email five weeks later.
On February 16, 2020, Mr. Bowen emailed FDA leadership, and copied Dr. Bright, stating: BARDA/HHS is the only government agency that understood that Americas fragile, foreign controlled mask and respirator supply was a national security problem. If theyd had the authority or if the VA and DOD had listened to them, BARDAs leaders, Rick Bright and Robinson, would have secured the mask supply. See email from M. Bowen to FDA (Feb. 16, 2020), attached hereto as Exhibit 29.
In late February 2020, as the number of confirmed positive COVID-19 cases in the United States approached 60, HHS leadership acknowledged that they were not prepared for a pandemic. When Secretary Azar testified before the Senate Appropriations Committee on February 25, 2020, he revealed that the SNS holds 30 million N95 respirators, yet Dr. Kadlec mentioned to the Senate this morning needing approximately 300 million for health care workers.(18) As calculated by previous FRMM reviews, the actual estimated number of disposable N95 respirators to protect healthcare workers in a pandemic response approached 3.5 billion over ten times the number Dr. Kadlec represented was necessary, and over 100 times the number available in the SNS. The following day, five weeks after Dr. Bright first urged immediate action to prevent a mask shortage, ASPR finally put out a pre-solicitation to collect information from mask producers to get information on where they might be able to buy N95 respirators and face masks. Three days later, the extent to which HHS officials underestimated the mask shortage became clear when the Surgeon General encouraged the public to stop buying masks, warning that a mask shortage could take important resources from health care professionals.(19) Following the ASPR SNS pre- solicitation notice to procure N95 masks, ASPR released a RFP to procure N95 respirators that closed on March 12, nearly two months after Dr. Bright began pushing for awareness and urgent action.
HHS leaderships refusal to heed Dr. Brights warnings about the shortage of needles and syringes to administer a potential vaccine was yet another serious point of tension between Dr. Bright and HHS leadership, including Dr. Kadlec. In January 2020, BARDA started forming partnerships to accelerate the development of vaccines to prevent COVID-19 illness and death. BARDA estimated that between 650 million and 850 million needles and syringes would be needed to administer a vaccine for the United States alone. Dr. Brights team further estimated that it could take up to two years to be able to produce enough of these supplies to deliver the vaccine. The SNS currently contains approximately 15 million needles and syringes, a mere 2% of the required amount. From late January through March 2020, Dr. Bright pushed the ASPR and Federal Emergency Management Agency (FEMA) supply chain groups to take swift and urgent action to place orders to secure limited supplies in the U.S., ramp up production, and begin stockpiling needles and syringes immediately.
— Footnotes —
18. See Jenni Fink, America has 30 Million Masks, Needs 300 Million for Health Care Workers Fighting Coronavirus, HHS Secretary Says, NEWSWEEK (Feb. 25, 2020), available at https://www.theinternetpatrol.com/brick-wall/ america-senate-committee-1489058.
19. See Maria Cramer, Surgeon General Urges the Public to Stop Buying Face Masks, NY TIMES (Feb. 29, 2020), available at https://web.archive.org/web/20230316112154/https://www.nytimes.com/2020/02/29/health/coronavirus-n95-face-masks.html.
— End of Footnotes —
During an HHS leadership call on March 13, 2020, Dr. Bright raised the issue with Dr. Kadlec directly, emphasizing the urgent need to halt the export of needles and syringes, place orders to buy, and ramp up production. Dr. Kadlec responded in a frustrated and dismissive manner, telling Dr. Bright that they should wait to act until they had something to inject. Dr. Bright pushed back, arguing that it was imperative to order the needles and syringes immediately to ensure that the United States would have them when a vaccine became available. As noted above, Dr. Bright raised concerns about this issue with Mr. Navarro during their meeting on February 14, 2020 and again in March. In turn, Mr. Navarro raised these issues to the White House Task Force. Dr. Bright and his team reiterated the dire consequences of these shortages and the need to take urgent action to begin stockpiling this life-saving equipment. Instead of heeding his recommendations, ASPR and FEMA staff sent Dr. Bright numerous emails indicating that there was a lack of clarity about which agency HHS or FEMA should buy the needles. In passing the buck back and forth, no group had yet placed orders for these critical supplies.(20)
Dr. Bright revisited the issue with HHS Leadership on March 12, 2020. He sent an email to Dr. Wolf, Mr. Adams, and SNS Director Kevin Cooper, advising them of the following:
[W]e are hearing rumblings about the US inventory of needles and syringes (critical ancillary supplies for vaccine and some therapeutics administration) are heading to other countries. There is a limited inventory in the supply chain, it could take 2+ years to make enough to satisfy the US vaccine needs for a pandemic. We need to hold on to all that we have and look at surging supplies now from producers.
See email from R. Bright to L. Wolf (Mar. 12, 2020), attached hereto as Exhibit 30. He ended the email by urging them to attend to this crucial supply issue so we are not chasing things down when we need them later and they are all procured by other countries. Id. Mr. Adams responded that he completely agreed with Dr. Brights concerns but the challenge may be finding the funding. Id. Dr. Bright then raised the issue directly with Dr. Kadlec, who again responded in a dismissive manner. Dr. Bright did not relent, however, and argued persistently for the need to order needles and syringes to have them available. Dr. Kadlec suggested that the needles and syringes could possibly be ordered in small tranches per month, instead of placing one large order.
— Footnotes —
20. In addition to identifying the need to purchase basic but critical supplies to administer the vaccine, Dr. Bright also raised concerns about a global shortage of glass vials that are required for vaccine production. According to major glass producers, all major pharmaceutical tubing suppliers are sold out of borosilicate tubing. It could take up to two years to produce enough vials for U.S. vaccine needs, while some therapeutics will also require vials. Dr. Bright advised leadership to devise an immediate strategy to address this critical shortage, to no avail.
— End of Footnotes —
To date, HHS has still not placed an order for these critical supplies. Lack of leadership and action by the ASPR SNS organization has placed the health and safety of all Americans at risk of not being protected from the deadly coronavirus even when a vaccine becomes available.
Between February and March, Dr. Bright met with Mr. Navarro six or seven more times. During each meeting, he briefed Mr. Navarro about drug supply issues and gaps in domestic drug manufacturing capacity, and his ongoing concerns about the shortages in masks, PPE for healthcare workers and first responders, needles and syringes, rapid handheld diagnostics, serology tests, vaccines, oral antiviral drugs and monoclonal antibodies for potential prophylactic use. After many of these meetings, Mr. Navarro sent memoranda to the White House Chief of Staff and Task Force members urging immediate action and implicitly criticizing HHS leadership for its failure to act. While Dr. Bright believed that the criticisms were warranted, he continued to try to handle these issues up his chain of command. Unfortunately, HHSs leadership acted with increased hostility towards Dr. Bright and made disparaging comments about the pressure they were receiving from Ricks friend in the White House. Ultimately, even the White House started referring to Dr. Kadlecs/ASPRs operation as a bottleneck. See email from P. Navarro to R. Kadlec (Mar. 19, 2020), attached hereto as Exhibit 31. This greatly angered Dr. Kadlec and his team, and led them to further marginalize Dr. Bright and to retaliate against him by pressing for his removal.
B. Dr. Bright Clashed with HHS Leadership About the Shortage of COVID-19 Testing Materials.
In addition to pushing HHS leadership to expand the mask supply, Dr. Bright also repeatedly urged HHS leadership to secure and expand the supply of COVID-19 testing materials, such as swabs to collect the virus specimen, Viral Transport Media (VTM) to transport the swabs to a laboratory, and chemical reagents to perform the test. On March 11, 2020, anticipating a shortage of these materials as testing ramped up around the country, Dr. Bright asked Mr. Adams for the SNSs inventory of chemical reagent, swabs, and VTM. See email from R. Bright to S. Adams (Mar. 11, 2020), attached hereto as Exhibit 32. To Dr. Brights surprise, Mr. Adams informed him that the SNS did not stock these items, and did not offer to assist in procuring them.
The next day, on March 12, 2020, Dr. Bright attended a hearing before the House Oversight and Reform Committee on coronavirus preparedness and response. During the hearing, CDC Director Dr. Robert R. Redfield testified repeatedly that the real challenge associated with implementing a national testing strategy would be supplying the requisite laboratory technicians, laboratory equipment, swabs, reagents, and other supplies necessary to perform the tests that already were in the marketplace. Dr. Redfield told the Committee, I want to really emphasize we focus so much on the actual test we have to focus now on the whole system to get that testing really rolled out. In listening to Dr. Redfields testimony, Dr. Bright grew increasingly concerned that there would be a severe shortage of testing materials, including swabs, as testing increased nationwide.
While sitting behind Dr. Redfield in the Congressional Hearing, Dr. Bright immediately instructed BARDA staff, including Deputy Director of Diagnostics and Medical Devices Rosemary Humes, to find out more about potential shortages and to compile a list of swab manufacturers in the event they needed to shore up the U.S. supply. He also sent an email to Dr. Johnson and Dr. Disbrow stating, I need details on reagents [in] short supply. And swabs in short supply. See email from R. Bright to R. Johnson (Mar. 12, 2020), attached hereto as Exhibit 33. Dr. Johnson responded in part, We heard you and are working on this. . . . everyone Im talking to says there is no swab shortage[.] Id. Dr. Disbrow likewise responded in part, Two people have indicated that [information regarding a swab shortage] may not be correct. Who has stated that there is an issue[?] See email from R. Bright to G. Disbrow (Mar. 12, 2020), attached hereto as Exhibit 34. Despite Dr. Johnsons and Dr. Disbrows skepticism about the impending shortages, Dr. Bright persisted. He told them, They [at the CDC] are referencing shortage of reagents. Shortage of swabs. Shortage of people in the labs, and urged them, Forget about shortage terminology. What swab options do we have[?] Where are they made? Id.
Early on the afternoon of March 12, 2020, Ms. Humes informed Dr. Bright that the CDC had confirmed that some [testing] sites are reporting that supplies are getting low, but that the FDA had assigned the matter to a shortages team, and the team did not anticipate a shortage of swabs because the two primary manufacturers had huge manufacturing capacity. See email from R. Humes to R. Bright (Mar. 12, 2020), attached hereto as Exhibit 35. Dr. Bright and Dr. Disbrow then called FDA Director of the Center for Devices and Radiological Health, Dr. Jeffrey Shuren, to learn where the FDA purchased its swabs. To Dr. Brights dismay, Dr. Shuren informed them that the FDA purchased its swabs from a manufacturer located in the Lombardy region of Italy the epicenter of Italys coronavirus outbreak which had been placed under lockdown to prevent the spread of the virus. Dr. Bright and Dr. Disbrow immediately contacted the DOD Defense Threat Reduction Agency (DTRA), which assisted BARDA with the transport of vaccines from Germany to the U.S. during the Ebola epidemic, to determine whether military flights could be used to transport swabs from Italy to the U.S. in the event that commercial planes could not because of the lockdown. See email from D. Wolfe to G. Disbrow, (Mar. 12, 2020), attached hereto as Exhibit 36.
Early the next morning, on March 13, 2020, DOD DTRA Deputy Division Chief Major Jeffrey Froude informed Dr. Disbrow that a request for military assistance with transporting the swabs likely . . . will need to come from [Secretary Azar] through official channels given the complexities of this mission and location restrictions compared to the previous [Ebola] mission. See email from J. Froude to D. Disbrow (Mar. 13, 2020), attached hereto as Exhibit 37. Later that morning, DTRA Director of Chemical and Biological Technologies Dr. Ronald Hahn confirmed, [A] direct request from SEC HHS to SEC DEF would get this at the appropriate level for decision and quick execution. Id. Anticipating Dr. Kadlecs resistance to this plan given his hostility toward Dr. Brights prior efforts to shore up the U.S. mask supply, Dr. Disbrow responded, Th[is] definitely complicates the matter. We will continue to determine the [swab manufacturers] ability to obtain air freight from commercial [carrier]. Id. In the event that he and Dr. Bright were not able to secure Secretary Azars approval to partner with DOD, Dr. Disbrow also reached out to the SNS about its ability to assist with transporting the swabs. See email from G. Disbrow to S. Adams (Mar. 13, 2020), attached hereto as Exhibit 38.
That same day, Dr. Bright sent an email to Mr. Navarro to let him know that BARDA had discussed [VTM] and swab issues with FDA and was reviewing several options to reduce stress on global supply chain. See email from R. Bright to P. Navarro (Mar. 13, 2020), attached hereto as Exhibit 39. In his email, Dr. Bright stated, We need to reduce our vulnerability of accessing these critical materials [such as swabs and VTM] from outside the US. These little things that no one thinks about are killing us. Id.
As Dr. Disbrow rightly predicted, Dr. Kadlec was resistant to even discussing the swab transport plan that he and Dr. Bright were trying to arrange with DOD. During an ASPR leadership call that afternoon, Dr. Bright attempted to brief Dr. Kadlec on the imminent swab shortages and critical need to find alternate transportation in the event that commercial planes could not fly to Italy because of the lockdown. Dr. Kadlec aggressively shot him down and in a hostile tone said, I dont care about swabs. I dont want to hear about swabs. Move on. Even after Dr. Disbrow told Dr. Kadlec that they had secured an option to fly military planes into Italy if they were able to obtain Secretary Azars approval, Dr. Kadlec refused to discuss the matter. Since Dr. Bright and Dr. Disbrow would need Dr. Kadlecs support to seek the Secretarys approval for the military flights, they seemingly had reached a dead end that could have had dire public health consequences.
Determined to secure a safe, reliable air bridge to Italy before the U.S. experienced a critical shortage of testing swabs, Dr. Bright turned to Mr. Navarro, his ally in the White House. On March 14, 2020, Dr. Bright emailed White House Senior Policy Advisor Christopher Abbott, a member of Mr. Navarros staff, to facilitate communication with Secretary of Defense Mark Esper about approving the military flights through the DOD. See email from R. Bright to C. Abbott (Mar. 14, 2020), attached hereto as Exhibit 40. Mr. Navarros office worked quickly and secured Secretary Espers approval in a matter of hours. Approximately two hours later, Maj. Froude confirmed that DTRA was working to have a flight in the air as soon as tomorrow night. Later that evening, Dr. Bright emailed Mr. Navarro, You did something miraculous tonight to break through the wall and bureaucratic barrier that was stalling shipment from Italy to US. Four days of bureaucracy that you broke down in 5 minutes. See email from R. Bright to P. Navarro (Mar. 14, 2020), attached hereto as Exhibit 41. Dr. Bright also asked rhetorically, Why do we buy our critical supplies such as swabs from Italy instead of US producers[?] . . . In a global crisis, global supplies quickly become global shortages. Solution: Incentivize expansion of US produced ancillary medical supplies. Buy American to sustain the US capacity. Id.
As a result of Dr. Brights persistence in the face of Dr. Kadlecs hostility and opposition to his and Dr. Disbrows plan, BARDAs partnership with the military has been able to transport 25 million swabs to the United States to address the dire shortage of this critical medical supply. The swab transport has now transitioned from the military operation to commercial cargo flights on Fed Ex and continues today between Italy and the U.S. to deliver swabs for use in testing facilities across the country. Unfortunately for Dr. Bright, however, his actions also increased Dr. Kadlecs growing hostility toward him and his frustration over Dr. Brights insistence that HHS secure the U.S. supply of masks and other critical materials to combat the ongoing coronavirus pandemic.
C. Dr. Kadlec and his staff increasingly circumvented Dr. Bright and BARDA in order to direct money without regard to scientific merit.
When COVID-19 emerged as global health threat, Dr. Bright anticipated that BARDA, NIH, CDC, FDA, and DOD would all be inundated with proposals. To streamline the process and maximize efficiency, Dr. Bright created an interagency Medical Countermeasures Task Force (MCM TF) consisting of subject matter experts from each government agency to review COVID-specific science and requests for funding on an expedited and collaborative basis. This centralized, interagency process was set up to enable companies to discuss their science and data with multiple agencies at once and to enable the federal government to move quickly to identify and support proposals with the greatest potential to combat COVID-19. Dr. Bright announced the MCM TF and its dedicated online submissions portal, which was managed by BARDA, to over 1,400 participants on a call on January 30, 2020.(21)
In late February 2020, Dr. Disbrow and Dr. Johnson informed Dr. Bright that Mr. Clerici and the CEO of Drug Innovation Ventures at Emory University, Dr. George Painter, who previously had sought funding for EIDD-2801 as a cure all drug on the basis of extremely limited pre-clinical data, were once again seeking funding for the drug this time, as a treatment for COVID-19. Instead of submitting a funding request to the MCM TF, however, Dr. Painter and Mr. Clerici contacted ASPR Strategic Innovation and Emerging Technology Manager Joe Hamel, a personal friend of Dr. Kadlecs and the head of ASPR Next, an opaque funding program within ASPR that was established in August 2019 to fund products, equipment, and technology to assist with healthcare emergencies. This concerned Dr. Bright for several reasons. First, to Dr. Brights knowledge, Emory still had not completed the clinical trials for which it had received nearly $30 million in NIH and DOD funds. See supra section II.D. Therefore, technical experts lacked what they needed to evaluate the drug and ensure that it was safe. Second, Dr. Painter and Mr. Clerici were deliberately circumventing the MCM TF submissions process designed to streamline COVID-specific funding requests. Third, Dr. Painter and Mr. Clerici were requesting funding for a drug, EIDD-2801, from a program, ASPR Next, which was designed to fund products, equipment, and technology and did not have the resources or technical expertise to fund drug development.
As Dr. Bright investigated this issue further, BARDA Director of Contracts Management and Acquisitions, Joffrey Benford, advised him that some companies attempted to circumvent BARDAs (or the MCM TFs) rigorous scientific and contractual review process by submitting requests for funding to ASPR Next, which seemed to require only a few paragraphs of information as compared with the robust submissions required by BARDA. Further, ASPR Next did not appear to limit its consideration to proposals for products, equipment, and technology, as it was designed to do. Once an ASPR CO approved an ASPR Next proposal for funding, Joffrey learned that the CO would simply attempt to transfer it to a BARDA CO with instructions to fund the proposal sometimes, with BARDA funds. Dr. Bright and his deputies consistently instructed BARDA COs not to fund proposals that had not been submitted to BARDA solicitations, been reviewed by BARDA (MCM TF) subject matter experts, or had gone through the full scientific and business proposal vetting process. However, it was becoming increasingly clear to Dr. Bright and others that Dr. Kadlec and Mr. Hamel were using ASPR Next to circumvent the BARDA review process and to fund their pet projects, regardless of scientific merit. Dr. Brights efforts to safeguard the review process were doing little more than escalating tensions with Dr. Kadlec and members of his leadership team.
— Footnotes —
21. At the time of Dr. Brights involuntary transfer, more than 2,300 MCM TF proposals had been submitted to the special portal.
— End of Footnotes —
On April 2, 2020, HHS Deputy Chief of Staff for Policy Paul Mango telephoned Dr. Bright to discuss the status of several funding proposals that Mr. Mango said had been submitted to ASPR Next, including one submitted by Ridgeback Biotherapeutics LP (Ridgeback). Dr. Bright told Mr. Mango that he did not know the status of any of the proposals but would find out what he could from Mr. Hamel. Later that morning, Dr. Bright sent an email to Mr. Hamel requesting information about the process ASPR Next is using to solicit, review and respond to proposals, especially those related to COVID-19, so that they could remain fully aligned as the pressure to succeed and report out continues to grow. See email from R. Bright to J. Hamel (Apr. 2, 2020), attached hereto as Exhibit 42. Dr. Bright also requested information about the number of ASPR Nexts submissions, the categories of those submissions, and the number of awards made and pending on a regular interval, in order to keep Mr. Mango and their other colleagues informed about the programs activities. Id.
Later that afternoon or the following day, having not received a response from Mr. Hamel, Dr. Bright called ASPR Chief Science Advisor, Dr. Chris Hassell, in an effort to learn more about ASPR Nexts internal processes. Dr. Bright told Dr. Hassell about his phone call with Mr. Mango and asked what he knew about ASPR Next. Dr. Hassell told Dr. Bright that he did not know much about the program, but that it appeared to him that Mr. Hamel was running his own enterprise at ASPR Next with Dr. Kadlecs tacit approval. Dr. Hassell also told Dr. Bright that Dr. Kadlec frequently took phone calls directly from industry partners and agreed to fund their proposals without following the requisite review processes. Dr. Hassell said that he had even discussed the issue with ASPR Principal Deputy Assistant Dr. Keven Yeskey, who was angry about ASPR Nexts deviation from the requisite contracting protocol. Dr. Hassell disclosed that he sought to keep his distance from ASPR Next because he was concerned about its potentially illegal and unethical processes.
A few days later, on April 7, 2020, the CEO of Ridgeback, Wendy Holman, telephoned Mr. Benford, to discuss the funding proposal she had submitted to ASPR Next for a clinical trial that was scheduled to begin the following day. As Mr. Benford later learned, Ridgeback had partnered with Emory on EIDD-2801 development, and the two were working together to secure funding. Ms. Holman told Mr. Benford that Mr. Shuy had directed her to work with him (Mr. Benford) to secure approximately $100 million in pre-award funding because ASPR Next contracting staff were overwhelmed. As Ms. Holman stated in an email to Mr. Benford later that day, Dr. Kadlec had called her the previous evening to ask her to accelerate [the clinical trials] as fast as possible. See email from W. Holman to J. Benford (Apr. 7, 2020), attached hereto as Exhibit 43. The next day, Mr. Shuy directed Mr. Benford to fund the Ridgeback proposal as quickly as possible, and preferably within 24 hours.
Mr. Shuys directive raised several significant concerns about the award process. First, acquisition procedures for a contract award of Ridgebacks size required in-depth analyses that would take at least 10-20 days to complete. Second, Ridgeback had not followed the proper procedure for receiving BARDA funding. It failed to submit a BAA white paper or full proposal to the BARDA BAA. In fact, Ridgeback had not provided BARDA with any documentation of its request for funding. Third, a time-sensitive procurement of this size would strain BARDAs personnel resources, slowing down critical activities for COVID-related projects that had already received BARDA approval. Mr. Benford enumerated these concerns in an email to ASPR HCA Schuyler Eldridge on April 13, 2020. See email from J. Benford to S. Eldridge (Apr. 13, 2020), attached hereto as Exhibit 44. Ultimately, Mr. Benford forced Ridgeback to adhere to BARDAs rigorous review process. The award was not made prior to Dr. Brights departure from BARDA.
As made explicit in email exchanges, Dr. Kadlec and his subordinates viewed Dr. Bright as an obstacle to their efforts to move BARDA money around. With the subject line, Shameless, Dr. Hassell emailed Dr. Kadlec on March 14, 2020 about DOD researchers request that Dr. Kadlec fund a list of projects with money from BARDA: That was a shameless attempt to circumvent [the Office of the Secretary of Defense] and BARDA and appeal to you directly to fund [DOD projects]. See email from C. Hassell to R. Kadlec (Mar. 14, 2020), attached hereto as Exhibit 45. Dr. Hassells email explained that some of these projects were already submitted to MCM TF, and went on to state that the labs DOD is seeking to fund are in trouble for shady dealings, illegal accounting, and lack of accountability. Id.
Yet instead of suggesting that ASPR deny DODs request for funding, Dr. Hassell explicitly offered to help ASPR work around Dr. Bright to obtain the necessary approval. Referring to Dr. Bright by name (in an email on which he inadvertently copied Dr. Bright), Dr. Hassell wrote: I know we have some issues with Rick, then offered to talk with BARDA staff within the Division of CBRN (chemical, biological, radiological and nuclear threats) Medical, whom Dr. Hassell described as straight shooters. Dr. Hassell concluded the email by insisting he will keep [Dr. Kadlec] legal. Id. Over the next few days, Dr. Hassell discussed DOD funding requests with various BARDA staff, working around Dr. Bright in the process. The projects in question totaled over $100M.
D. Dr. Kadlecs animus toward Dr. Bright escalated markedly when Congress for the first time appropriated money directly to BARDA, making it harder for him to siphon off and control BARDAs funds.
In early to mid-March 2020, HHS legislative officers received requests for Dr. Bright and Dr. Disbrow to brief various members of Congress and staff, including from the House Appropriations Committee, regarding BARDAs efforts to combat COVID-19, which they did. At the same time, Dr. Bright received calls directly from members of Congress or their staff, including from Senator Steve Daines (R-MT), Senator Chris Coons (D-CT), Senator Roy Blunt (R-MO), Congresswoman Anna Eshoo (D-CA) and a staff member in the office of Congresswoman Rosa DeLauro (D-CT). During each of these conversations, Dr. Bright explained how BARDA used its funds to aggressively support possible COVID-19 treatments, diagnostics, and vaccines. He also explained that BARDA had not been able to move as quickly as he would have liked because it lacked money, experienced delays in accessing funding once appropriated, and was receiving more proposals than it could fund. Dr. Bright also explained that HHS and ASPR had siphoned off some of the money Congress had designated for drug and vaccine development, leaving BARDA in a position where it had to plead with Dr. Kadlec and Secretary Azar for the money it needed to do its job.
On March 20, 2020, Dr. Bright spoke with Senator Daines about BARDAs efforts to combat the pandemic. Senator Daines emphasized the importance of BARDAs work, and said something to the effect of, The last thing we want to do is have you worry about money when you should be focusing on science.
Around this same time, Dr. Kadlec learned of the possibility of a direct congressional appropriation to BARDA, rather than through HHS/ASPR, and he was furious. On March 20, he emailed Dr. Bright: BTW did you ask Eshoo to find (sic) BARDA over ASPR?! See email from R. Kadlec to R. Bright (Mar. 20, 2020), attached hereto as Exhibit 46. In response, Dr. Bright explained that earlier that day, Senator Daines asked BARDA for a huge back of envelope estimate to pull out all stops for vaccine and drugs, and he [w]ants a huge number by this afternoon. Id. Dr. Bright said that Dr. Disbrow and Dr. Johnson were working on preparing these estimates. One minute later, Dr. Kadlec responded, Shuy needs to review ALL such estimates and submissions. Id. Dr. Bright replied that he understood, and that Dr. Disbrow would be sending an estimate soon. Mr. Shuy then separately asked to connect with Dr. Bright offline. He instructed Dr. Bright, Do not reach back out to these [congressional] offices or staff at this time. Id.
On March 27, 2020, Congress passed and President Trump signed the Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub. L. 116136. The Act appropriated $3.5 billion directly to BARDA for expenses related to the manufacturing and production of vaccines, therapeutics, and diagnostics responsive to COVID-19. To Dr. Brights knowledge, this was the first time Congress appropriated money directly to BARDA and it was a game changer.(22) For the first time, the ASPR had less control over BARDAs money, and BARDA could direct its resources towards those proposals with the greatest scientific potential to combat COVID-19. Accordingly, it became much more difficult for Dr. Kadlec to redirect funds to support projects for his cronies or for political purposes. Dr. Kadlec obviously understood this fact and was not happy. After the passage of the CARES Act, Dr. Bright did not see or speak with Dr. Kadlec until three days later, on March 30, 2020. On that date, Dr. Bright entered Dr. Kadlecs office at FEMA headquarters and attempted to update him on a new initiative being planned to rapidly enable a serology/antibody testing program. Dr. Kadlec sat in a chair working on his laptop and did not look up. Dr. Bright nevertheless provided Dr. Kadlec with an overview of the program and mentioned a potential briefing to Secretary Azar that evening or the next day. Dr. Kadlec responses were monosyllabic ok sure ok. He never looked up from his computer and his demeanor was dismissive and disrespectful.
— Footnotes —
22. Previously, Congress appropriated money to HHS, and the Secretary of HHS managed the availability and distribution of the funding. Prior to passage of the CARES Act, the HHS Assistant Secretary for Financial Resources (ASFR) was able to transfer funds to the ASPR, who in turn could transfer funds to BARDA. To receive money, BARDA had to submit a spending plan to Dr. Kadlecs budget officer, Jay Petillo, who in turn submitted the plan to the ASFR. Through this process, Dr. Kadlec had complete control over BARDAs money, and the ASFR oversaw the overall budget process for the department. Accordingly, both the Secretary of HHS and the ASPR, Dr. Kadlec, could control how much money BARDA received and when they received it, and also had the authority to transfer money out of BARDAs account. In fact, on multiple occasions, Dr. Kadlec directed Mr. Petillo to transfer money out of BARDAs account, often to the SNS or to support projects for ASPR Next, despite Dr. Brights objections. See e.g., section II(B), supra.
— End of Footnotes —
E. Dr. Kadlec tried to bypass Dr. Bright to access BARDA money over Dr. Brights objections.
On March 20, 2020, Dr. Kadlec wrote to the Executive Vice President of Research at Northwell Health, Dr. Kevin Tracey, to request an expedited review of the companys clinical trial to develop a COVID-19 treatment. See letter from R. Kadlec to K. Tracey (Mar. 20, 2020), attached hereto as Exhibit 47. Northwell Health was working with Alchem Laboratories (Alchem) on a treatment using hydroxychloroquine in combination with famotidine, the active compound in the heartburn drug Pepcid AC. Dr. Kadlec invited Northwell Health to submit a proposal to ASPR Next and, in an unprecedented move, instructed it to work with COVID clinical expert, Dr. Michael Callahan, in the preparation of this white paper and draft budget. Id. Dr. Callahan is a consultant on Dr. Kadlecs staff who was hired to advise HHS about the governments COVID response. He is not a government employee. Yet as a consultant who is advising or has advised the Federal Government with respect[] to a Federal agency procurement, Dr. Callahan is prohibited from disclosing information about a contractor bid or proposal, or source selection information, before the award of a Federal agency procurement contract. See 41 U.S.C. 2102(a)(3)(A). By directing a member of his staff to work as an agent of both the company and the government regarding the proposal, Dr. Kadlec was inviting violations of federal procurement law.
On March 31, 2020, Dr. Tracey emailed a proposal and budget to Dr. Kadlec for Northwell Health, also confirming that he had worked with Dr. Callahan to prepare the submission for BARDA.(23) Dr. Tracey copied Secretary Azar, and other HHS senior officials, but not Dr. Bright on this email. See email from K. Tracey to R. Kadlec (Mar. 31, 2020), attached hereto as Exhibit 48. Within an hour, Dr. Kadlec responded in part: I have actioned this with BARDA [sic] Michael Callahan will follow up. Id. Although Dr. Kadlec communicated with Dr. Disbrow about the proposal, he did not notify Dr. Bright.
Dr. Bright learned about this proposal when someone on the email exchange forwarded the messages to him, Dr. Disbrow, and others, along with the note: FYSA no one from BARDA or the MCM TF is copied on this plan for an expanded access Clinical Trial, but they are asking if it will be transferring to BARDA after award by ASPR Next. Id. On or around April 1, 2020, Dr. Disbrow called Dr. Bright with concerns about this request. Dr. Disbrow asked Dr. Bright, Can you believe they want to use Pepcid AC now? Dr. Disbrow noted that this was a Callahan thing. Dr. Bright told Dr. Disbrow that Dr. Callahans involvement seemed to be a conflict of interest, and Dr. Disbrow agreed. Afterward, Dr. Bright called Dr. Linda Lambert, who oversees the BARDA clinical team, to discuss his concerns about this contract proposal and Dr. Callahans role in assisting companies with their contract submissions. Dr. Lambert was also concerned about the contract proposal, and agreed with Dr. Bright that Dr. Callahans involvement was a conflict of interest. Dr. Bright instructed Dr. Lambert to ensure that BARDA had a clinical review of this drug. On April 1, 2020, Dr. Disbrow sent an email directing relevant BARDA employees to pause on further emails since no actual proposal has been submitted. See id.
— Footnotes —
23. See Brendan Borrell, New York Clinical Trial Quietly Tests Heartburn Remedy Against Coronavirus, SCIENCE (Apr. 26, 2020), available at https://www.sciencemag.org/news/2020/04/new- york-clinical-trial-quietly-tests-heartburn-remedy-against-coronavirus (detailing Dr. Callahans simultaneous work with Dr. Kadlec and Northwell Health to obtain BARDA award).
— End of Footnotes —
Three days later, Dr. Kadlec again excluded Dr. Bright when he emailed senior BARDA officials directing the award of BARDA funds to Northwell Health. On April 4, 2020, Dr. Kadlec sent an email to Dr. Disbrow and Dr. Lambert encouraging them to move forward with the proposal: Gary and Linda just following up on this and making sure we support this trial. I understand there was some follow up to determine the exact cost of this. But would like to close the loop on this. See email from R. Kadlec to G. Disbrow (Apr. 4, 2020), attached hereto as Exhibit 49. On April 14, 2020, BARDA awarded Alchem a $20.7 million contract for work to be performed by Northwell Health. Dr. Bright, the BARDA Director, was entirely excluded by Dr. Kadlec from the award process on this contract.
This contract was just one more example of Dr. Kadlecs actions in bypassing all rules and procedures designed to ensure public safety and to avoid corruption in the award of billions of dollars in government funds. Indeed, Dr. Kadlec cultivated an environment in which industry partners regularly bypassed agency procedures designed to prevent influence peddling and conflicts of interest, forcing Dr. Bright and his deputies to spend valuable timeincluding during the ongoing COVID-19 health crisisfending off improper and often illegal requests from private industry and their agents.
Most recently, on April 10, 2020, Novavax CEO Stanley Erck called Dr. Brights office requesting to speak directly with Dr. Bright about Novavaxs proposal for a COVID-19 vaccine. Since Novavax had already submitted a BAA white paper about the vaccine, federal law clearly prohibited Dr. Bright from speaking with him about the companys proposal. Dr. Brights Special Assistant therefore informed Mr. Erck that BARDA could not discuss the proposal at that time. Undeterred, three days later on April 13, 2020, Novavax Senior Vice President of Public Policy and Commercial Strategy Brian Rosen circumvented Dr. Brights office entirely and sent an email directly to Dr. Kadlec. In his email, Mr. Rosen touted Novavaxs history of working with coronaviruses, provided information about recent milestones in the companys development of its COVID-19 vaccine, and lauded the vaccine as one of the earliest and most promising. He also requested an opportunity to speak with directly with Dr. Kadlec about the companys proposal. See email from B. Rosen to R. Kadlec (Apr. 13, 2020), attached hereto as Exhibit 50.
Soon after learning about Novavaxs second attempt to circumvent federal law and speak with Dr. Bright or Dr. Kadlec, Dr. Disbrow emailed Dr. Hassell, Dr. Houchens, and Dr. Bright stating in part, we cannot have discussions with [Novavax] with respect to their [BAA white paper] submission. All submissions will be reviewed by the [MCM TF] for prioritization. Id. Dr. Bright responded that [d]ue to the nature of having an open proposal in house, I strongly encourage you [Mr. Hassell] to coordinate with the ASPR [Head of Contracting Activity (HCA)], Schuyler Eldridge, to determine the best way to handle this call with ASPR.(24) Id. In stark contrast to the approach of Dr. Bright and Dr. Disbrow, and despite the fact that speaking with Mr. Erck or Mr. Rosen about Novavaxs pending submission was a blatant violation of federal law, Dr. Kadlec responded to Mr. Rosens email that he was looking forward to speaking with him. See email from R. Kadlec to B. Rosen (Apr. 13, 2020), attached hereto as Exhibit 51. Dr. Bright, who received notice of his removal just four days later, does not know whether Dr. Kadlec ultimately spoke to Novavax about its proposal but assumes that he did so. This of course warrants further inquiry.
F. Dr. Bright resisted pressure from HHS leadership to make potentially harmful drugs widely available, including chloroquine and hydroxychloroquine, and provided information to a reporter about the specific danger to the public health and safety caused by the Administrations decision to release these untested drugs for use by the general public.
In an apparent effort to score a short-term political victory for the Administration during the escalating health crisis, the Office of the ASPR pressured BARDA to promote the malaria drug chloroquine as a therapeutic for COVID-19, despite a clear lack of scientific support. On March 10, 2020, ASPR Chief of Staff Shuy emailed Dr. Johnson, who was head of BARDAs Division of Influenza and Infectious Diseases, to ask whether BARDA was considering chloroquine as a therapeutic for COVID-19. See email from B. Shuy to R. Johnson (Mar. 10, 2020), attached hereto as Exhibit 52. Under BARDAs COVID-specific contract approval process, Dr. Johnson was then serving as SSA with final approval over BARDAs COVID-19 related contracts with private industry. Dr. Johnson responded to Mr. Shuy that the MCM TF was monitoring clinical trials of the drug, but it was not enthusiastic about chloroquines use as a therapeutic. Specifically, Dr. Johnson told to Mr. Shuy that although the drug has been shown to have in vitro effects on other microbes…that has not panned out to clinical benefit for COVID-19 patients. Id.
On March 17, 2020, and without explanation, Mr. Shuy demanded an update from Dr. Johnson about the use of chloroquine as a therapeutic for COVID-19. Mr. Shuy wanted the information ASAP . . . like immediately [.] Id. Dr. Johnson responded by reiterating the scientific basis for the MCM TFs lack of enthusiasm about the drug i.e., the data to date was not compelling but assured Mr. Shuy that the MCM TF was closely monitoring several ongoing clinical trials of the drug. Id. That afternoon, Joseph Hamel, ASPR Strategic Innovation and Emerging Technology Manager, emailed BARDA Acting Director of CBRN Medical Countermeasures and lead for the COVID-19 MCM TF, Dr. Christopher Houchens, and several ASPR officials stating that an outside group had approached the ASPR about a promising compound for the treatment of COVID-19: chloroquine. See email from J. Hamel to C. Houchens (Mar. 17, 2020), attached hereto as Exhibit 53. According to Mr. Hamel, Bayer AG (Bayer) had offered to donate three million chloroquine pills to the SNS. Mr. Hamel directed Dr. Houchens to have his team take a look at safety information provided by Bayer to make sure its legit. Id. Mr. Hamel closed his email by stating, This can be a BIG immediate win. Id. (Emphasis added).
— Footnotes —
24. As the ASPR HCA, Mr. Eldridge is charged with enforcement of the federal law at issue, the Procurement Integrity Act (PIA).
— End of Footnotes —
Unfortunately, the scientific evaluations did not support the utility of the Bayer donations. Later on March 17, 2020, Dr. Houchens emailed Dr. Bright with his teams review of Bayers chloroquine safety information. See email from C. Houchens to R. Bright (Mar. 17, 2020), attached hereto as Exhibit 54. The email communicated his teams opinion that there are safety liabilities associated with the drug…accepting the donation could send a signal that we are not concerned about the risk. Id. (Emphasis added). He stasted (sic): I do not believe we should accept the donation [of chloroquine from Bayer] until we have an understanding on the clinical utility of the drug. Accepting the donation could lead to widespread use that is not supported by any clinical data. Id. (Emphasis added). Dr. Houchens noted that not a single study has posted any data for peer-review and he emphasized that [w]e need to be very careful about the message it sends the public about accepting a donation of a drug with questionable utility …. Id.
Dr. Bright received a similar message from BARDA Chief of Therapeutics for Influenza and Emerging Infectious Diseases and Lead for the COVID-19 therapeutics working group within MCM TF, Dr. Kimberly Armstrong, who stated that the consensus among BARDA and FDA scientists was to wait for additional clinical data before making any recommendations on the use of chloroquine to treat COVID-19. See email from K. Armstrong to R. Bright (Mar. 17, 2020), attached hereto as Exhibit 55. Dr. Armstrong expressly stated that there was no data available to support that chloroquine provides clinical benefit in the treatment or prevention of COVID-19. Id. (Emphasis added).
The next day, March 18, 2020, Dr. Bright wrote Mr. Hamel that it remained unclear what ASPR has in mind with this donation plan and requested from Mr. Hamel all information and data received about the Bayer donation and all prior discussions with Bayer. See email from R. Bright to J. Hamel (Mar. 18, 2020), attached hereto as Exhibit 56. Mr. Hamel told Dr. Bright to direct any questions to Mr. Shuy, who he said was running point on coordinating the donation with Secretary Azar and Bayer. Id. Also on March 18, 2020, Mr. Hamel emailed Dr. Johnson and SNS officials at ASPR that he had [j]ust got[ten] the call from Bryan [Shuy] and it was [t]ime to move on obtaining an Emergency Use Declaration. See email from J. Hamel to R. Johnson (Mar. 18, 2020), attached hereto as Exhibit 57. An Emergency Use Declaration enables the FDA to issue an Emergency Use Authorization (EUA), which allows unapproved drugs, or unapproved uses of approved drugs, to be used in an emergency when there are no adequate, approved, and available alternatives. A chloroquine EUA would make the drug available for the treatment of COVID-19 under a physicians supervision in a hospital setting. That afternoon, and prior to the ASPRs official approval, Axios reported that Bayer was preparing to donate a large supply of an older malaria drug, chloroquine, to the SNS.(25)
— Footnotes —
25. Caitlin Owens, Scoop: Bayer to Donate Potential Coronavirus Drug to U.S., AXIOS (Mar. 18, 2020), available at https://www.theinternetpatrol.com/brick-wall/ cc8c1a5a-6a14-4e36-8b07-07eccf4eff36.html.
— End of Footnotes —
The next day, on March 19, 2020, Bayer announced that it had in recent days . . . been in talks with the White House, HHS, CDC, and the FDA and planned to join the U.S. governments fight against COVID-19 by donating three million tablets of chloroquine to the SNS.(26) The press release stated that chloroquine was FDA-approved for the prevention and treatment of malaria but had shown limited potential for the treatment of COVID-19. The press release also stated that Bayer was working with appropriate agencies on an Emergency Use Authorization so that the drug could be used to treat COVID-19 in the U.S. That same day, President Trump falsely stated during a White House press conference that clinical trials of chloroquine and/or hydroxychloroquine were producing very, very encouraging early results and promised the American public that his Administration was going to be able to make [chloroquine and/or hydroxychloroquine] available almost immediately.(27)
Over the next several days, HHS, ASPR, and FDA facilitated the importation of Bayers donation of chloroquine from manufacturers and distributors in Pakistan and India and also sourced chloroquine and hydroxychloroquine from domestic manufacturers to shore up the U.S. supply. During this time, however, it remained unclear to Dr. Bright and others at BARDA how the drugs would be made available to the public, including which agency would sponsor the widely-publicized EUA.
On March 23, 2020, Dr. Bright received an urgent directive from HHS General Counsel Bob Charrow, passed down from the White House, to drop everything and make the chloroquine donated by Bayer widely available to the American public. Mr. Charrow told Dr. Bright that Secretary Azar was directing BARDA to establish a Nationwide Expanded Access Investigational New Drug (IND) protocol for chloroquine, which would provide significantly greater access to the drug than would an EUA. Mr. Charrow told him that the protocol was to include a new database or application created by Oracle to assist in determining who got the medicine and to allow patients to enter their symptoms into an app in lieu of seeing a physician while taking the drug. Unlike an EUA, a Nationwide Expanded Access IND protocol would make the drug available for the treatment of COVID-19 outside a hospital setting and without close physician supervision. According to Mr. Charrow, Secretary Azar was issuing the directive to accommodate both the Bayer donation of chloroquine tablets and a soon-to-be-announced donation by Oracle co-founder Larry Ellison of an online platform about which Mr. Charrow could provide few details. Media reports from the time period indicate that Mr. Ellison, a prominent Trump donor, helped convince President Trump that chloroquine and hydroxychloroquine could effectively treat COVID-19.(28)
— Footnotes —
26. Bayer Partners with U.S. Government on Major Product Donation to Fight Coronavirus, BAYER (Mar. 18, 2020), available at https://www.theinternetpatrol.com/brick-wall/ Partners-with-US-Government-on-Major-Product-Donation-to-Fight-Coronavirus/default.aspx.
27. See Remarks by President Trump, Vice President Pence, and Members of the Coronavirus Task Force in Press Briefing, WHITE HOUSE (Mar. 19, 2020), available at https://www.theinternetpatrol.com/brick-wall/ members-coronavirus-task-force-press-briefing-6/.
28. See, e.g., Yasmeen Abutaleb, et al., Oracle to Partner with Trump Administration to Collect Data on Unproven Drugs to Treat COVID-19, WASH POST (Mar. 24, 2020), available at https://www.theinternetpatrol.com/brick-wall/ e4ce3fbd85b5_story.html.
— End of Footnotes —
Mr. Charrow also told Dr. Bright that he had personally drafted the informed consent form required for the Expanded Access IND protocol and wanted BARDA to set up this program within the next two days. Mr. Charrow further advised Dr. Bright that the donated drug was to be deposited in the SNS for distribution to Americans. Dr. Bright later learned that neither the foreign drug production facilities, nor the pills, had been inspected by the FDA or approved for safe use in the United States.
Secretary Azars directive concerned Dr. Bright for several reasons: first, the best scientists and clinicians in HHS had advised that data on chloroquine and hydroxychloroquine was insufficient to know if these drugs had any clinical benefit in COVID-19 patients; second, there were known safety concerns associated with these drugs, including dangerous irregular heart rhythms and even fatalitiesrisks that could increase if the drugs were used in combination with other drugs, including some antibiotics; and third, inconsistent and often dangerous lapses in quality control in some non-FDA inspected drug production facilities raised concerns of potential toxicity posed by contaminants and uncontrolled levels of active ingredients in imported medicines. Given the growing panic over the COVID-19 pandemic, the desperation to find a cure, and the irresponsible public promotion of an unproven medicine, Dr. Bright was extremely concerned about the prospect of chloroquine being made readily available to the public, without close patient monitoring by medical professionals. HHS scientists repeatedly agreed that the best path forward would be to evaluate chloroquine and hydroxychloroquine through randomized, placebo-controlled clinical trials (RCT), which were already underway.
Secretary Azars directive to secure a Nationwide Expanded Access IND protocol for chloroquine based on scant scientific evidence and on such a short timeframe sent Dr. Bright and his colleagues scrambling. Within the hour, Dr. Bright had called a meeting of Dr. Linda Lambert, Chief Medical Officer Dr. Robert Walker, Director of Regulatory and Quality Affairs Dr. Tremel Faison, and Drs. Johnson, Disbrow, and Houchens to discuss the directive. The group expressed serious concerns about a Nationwide Expanded Access IND protocol for chloroquine given the lack of clinical data available about its therapeutic benefits and concerns about its potential safety risks, especially if administered without close physician supervision. Dr. Bright and FDA colleagues were also concerned about the quality and potential toxicity of chloroquine supplies produced and shipped in from facilities in India and Pakistan that were not approved by the FDA, and were therefore not approved to be used in the U.S. marketplace. The HHS clinical and regulatory expert teams worked frantically for 48 hours without sleep to come up with a plan that would ensure the greatest level of safety for people who received this drug. They discussed narrower options for the rollout, including a small pilot study, and established an interagency working group of clinical and regulatory experts to determine the safest way to make the unproven drug available without causing harm to the American public.
Later that same day, March 23, 2020, FDA Chief Counsel Stacy Amin urged various HHS and FDA officials to move forward on the Expanded Access IND protocol for chloroquine to coincide with President Trumps forthcoming announcement of his Administrations partnership with Oracle. See email from S. Amin to R. Charrow (Mar. 23, 2020), attached hereto as Exhibit 58 (Can we please start moving forward on BARDA sponsoring the chloroquine IND and NIH providing the IND (sic) ? The President is announcing this tonight and I believe the WH would like it set up by tomorrow with data to flow into the Oracle platform.) Dr. Bright remained extremely concerned, as HHS leadership seemed willing to make these drugs widely available without any clinical assurance that the drug was safe. He feared that the wide scale availability of chloroquine and hydroxychloroquine could lead to serious patient harm and potentially many patient deaths.
In an email to Dr. Kadlec and several of Dr. Brights BARDA colleagues that evening, Dr. Bright expressed frustration with BARDAs exclusion from the decision-making process, stating, I am not sure who has the background on this, BARDA does not yet and [is] playing catch up with little to no details. … Who has talked with Oracle? Where is the drug coming from? Has FDA cleared? Id. In response, Dr. Kadlec merely confirmed what Dr. Bright already knew: Bob Charrow asked that BARDA lead this. Please identify a team to support. Id.
That night, Dr. Bright emailed Ms. Amin stating that the details available to BARDA regarding an Expanded Access IND protocol for chloroquine remained very sketchy, even though the Secretary had directed BARDA to move quickly. See email from R. Bright to S. Amin (Mar. 23, 2020), attached hereto as Exhibit 59. He requested to speak with Ms. Amin urgently about the Secretarys directive. Ms. Amin responded that the White House planned to discuss the following morning whether the protocol should be national in scale or piloted to New York first. Dr. Bright replied, in part: Given the limited information we have on both the drug and the innovative data system, Im sure wed all lean heavily towards a pilot over a national rollout. Many variables to get right in an already hectic setting across the nation. Id.
The next day, on March 24, 2020, the Director of the Center for Drug Evaluation and Research, Dr. Janet Woodcock, called Dr. Bright and strongly recommended that BARDA submit an application for an EUA instead of an Expanded Access IND protocol. Given the uncertainty about the risks of chloroquine, an EUA would better protect patients by enabling physicians to closely monitor their progress in a hospital setting and treat any side effects of the drug. Dr. Bright agreed with Dr. Woodcock that more limitations on these unknown drugs would be safer for the American public. A small Chinese clinical study released that same day, and which Dr. Bright discussed with Dr. Woodcock, produced statistically insignificant results about the therapeutic benefits of hydroxychloroquine and provided no more compelling reason to make the drug available nationwide without also requiring the close supervision of a physician when administered.
Over the next several days, Dr. Bright and Dr. Woodcock urged their colleagues on the clinical and regulatory teams implementing the Secretarys directive to secure an EUA for chloroquine and hydroxychloroquine instead of a Nationwide Expanded Access IND protocol. Implementing the EUA was a compromise position, to rein in HHS leaderships initial campaign to make the drugs available to the public outside of a hospital setting and without physician supervision. Dr. Bright and Dr. Woodcock ultimately prevailed upon their colleagues, and the FDA assisted BARDA in drafting an EUA request and provided it to Dr. Bright on the evening of March 28, 2020. Dr. Bright reviewed and edited the request letter to clarify that although he was being directed to sign the EUA request, it was not at his or BARDAs behest. After Dr. Kadlecs review and approval, the EUA request was sent to the FDA at 11:31p.m. on March 28, and at 12:03 a.m. on March 29, 2020, the FDA issued an EUA for chloroquine and hydroxychloroquine to be used by licensed health care providers to treat adults and teens hospitalized with confirmed COVID-19 who weigh more than 110 pounds, if they could not otherwise participate in a randomized controlled trial. This directivewhich kept chloroquine and hydroxychloroquine in the hands of healthcare professionals, and out of the hands of the public at largeensured that the drugs were administered to patients only under close physician supervision and who were known to be infected with the virus.
Despite the brokered compromise, the Administration nevertheless continued to push for expanded, unsupervised access to chloroquine and hydroxychloroquine, in blatant violation of the EUA issued by its own FDA and regardless of the risk to the American public. On April 4, 2020, hours after President Trump once again touted hydroxychloroquine as a treatment for COVID-19 during a White House press conference, HHS Assistant Secretary for Health Adm. Brett Giroir, M.D., instructed FEMA Administrator Peter Gaynor, Vice Director for Logistics of the Joint Chiefs of Staff Rear Adm. John Polowczyk, and Dr. Kadlec to mobilize the nations supply chain to flood NY and NJ with treatment courses [of hydroxychloroquine]. See email from B. Giroir to S. Adams (Apr. 4, 2020), attached hereto as Exhibit 60. Admiral Giroir issued this instruction based on orders from the White House. Mr. Gaynor likewise had received instructions from FDA Commissioner Dr. Stephen Hahn to distribute hydroxychloroquine to pharmacies nationwide, even though the EUA did not provide for outpatient use of the drug.
When SNS Deputy Director Steven Adams cautioned Admiral Giroir that the EUA limits the use of chloroquine and hydroxychloroquine to the treatment of hospitalized patients, he responded, NOPE …Needs to go to pharmacies as well. The EUA matters not …The drug is approved [and] therefore can be prescribed as per doctors orders. That is a FINAL ANSWER. Id. (Emphasis added). Adm. Giroirs response made crystal clear that the Administration would stop at nothing to make the experimental drug widely available to the American people, no matter the consequencesnot because it was safe or effective, but because as ASPRs Joe Hamel stated, it was seen by the Administration as a BIG immediate win.
At this point, Dr. Bright had exhausted all efforts to protect patients from the Administrations embrace of hydroxychloroquine and chloroquine as a treatment for COVID-19. He believed the EUA he had brokered would limit the administration of the drugs to patients in a hospital setting and under the care of physicians. Yet the following week, the Administration, including the Dr. Kadlec, had continued to push chloroquine and hydroxychloroquine for widespread use in non-clinical settings and without physician supervision. Dr. Bright remained extremely concerned about the drugs importation from Pakistan and India because the FDA had not inspected the drugs or the factory that produced them. In Dr. Brights experience, drugs from uninspected factories can be contaminated or dosed improperly, and this could obviously be dangerous to those who took the medication. Apparently unconcerned about this known danger, Dr. Kadlec and others in the Administration sought to flood the marketplace with these drugs. Dr. Bright and his staff voiced their concerns repeatedly, but the Administration was not interested in hearing from BARDA or the MCM TF the subject matter experts. Dr. Bright and his team had apparently spent all their political capital in their effort to limit chloroquine and hydroxychloroquine to an EUA. Within HHS, there was no desire (outside of BARDA) to stop this speeding train. Dr. Bright felt powerless to protect the public from this potentially toxic chemical that HHS, at President Trumps insistence, was touting as a safe treatment.
Yet he felt an urgent and compelling need to inform the American public that this drug with insufficient scientific data to support its use for COVID-19 patients, with known safety concerns, and with no FDA oversight over its quality was now being pushed or flooded onto the streets of America. At this point, Dr. Bright felt that the government had failed to adequately heed these warnings and to inform Americans of the source and serious risks posed by this donated drug. He believed that Americans needed to have this critical information available to them to before taking the medication.
It was at this time that a journalist left a message for Dr. Bright inquiring about the potential dangers of hydroxychloroquine and chloroquine. The journalist indicated that numerous government sources had expressed concerns about the donated chloroquine coming from unregulated factories in India and Pakistan, that there were significant risks associated with these drugs, and that the administration was rushing to get them into the hands of the American people. The journalist asked Dr. Bright to confirm this information. Dr. Bright considered the request carefully. He felt that he had exhausted all avenues to alert government officials that they were rushing into a potentially dangerous situation and that there was no one to help stop the push to flood the country with this unproven and potentially dangerous drug. He concluded that his only remaining avenue was to share his concerns with the journalist who understood the specific issue and risks associated with these drugs and who had already gathered substantial information from multiple sources.
In coming to this decision, Dr. Bright wrestled with what he felt was both a moral and a professional obligation to save lives and protect Americans. He knew that providing this information to a journalist would place him further at odds with HHS leadership. However as the death toll mounted exponentially each day, Dr. Bright concluded he was left with no choice, and he had a clear obligation to the American public, particularly those vulnerable as a result of illness from COVID-19, to protect it from drugs which he firmly believed constituted a substantial and specific danger to public health and public safety. Dr. Bright gave the journalist HHS emails that were not privileged or classified or otherwise legally restricted from dissemination, which discussed the drugs potential toxicity and demonstrated the political pressure to rush the drugs from Pakistan and India to American households.(29) Dr. Bright hoped that by shining a light on HHSs reckless and dangerous push to make these drug available, human lives would be saved. On April 15, 2020, with rumors of an upcoming article circulating at HHS, Mr. Shuy brought up the media, and specifically warned him to be careful about speaking to the media.
— Footnotes —
29. Dr. Brights disclosures to the journalist are protected under the Whistleblower Protection Act (WPA), 5 U.S.C. 2302(b)(8)(A) (protecting employees who disclose information that reveals any violation of any law, rule, or regulation, or a substantial and specific danger to public health or safety); Department of Homeland Security v. MacLean, 574 U.S. 383, 393 (2015) (federal employees disclosures to reporter about dangerous agency activity were protected under Whistleblower Protection Act) (citing 5 U.S.C. 2302(b)(8)(A)).
— End of Footnotes —
When an article later appeared that demonstrated the reckless actions of the Administration to release an unproven and potentially very dangerous drug, HHS leadership suspected that Dr. Bright was the source. The article did not reflect well on the Administration as it made clear that officials were well aware of the potentially serious issues with the drug but nevertheless viewed it as a political win. Following Dr. Brights removal as Director of BARDA and involuntary transfer, HHS officials told the media that Dr. Brights relationship with Dr. Kadlec had been frayed, but the leak was the straw that broke the camels back.(30)
G. Dr. Bright achieved significant success as Director of BARDA and his removal was blatantly retaliatory.
On the morning of Friday, April 17, 2020, Dr. Bright briefed Senator Roy Blunt (R-MO) about BARDAs work on vaccines and drugs to address the COVID-19 pandemic. Senator Blunt was particularly interested in BARDAs diagnostic efforts, and Dr. Bright advised him about BARDAs plans to invest first in big laboratories to augment CDC capabilities, then rapidly push technology to get diagnostics closer to patients, simplify the testing, and to reduce the time it takes patients to get results. He told the Senator about BARDAs strategy that was created in mid- January to accelerate development of SARS-CoV-2 testing and its recent awards to companies developing home diagnostic tests and to companies developing both antigen and antibody tests a key to getting Americans back to work. Senator Blunt was impressed with Dr. Brights briefing and told him that he was proud of Dr. Bright and of BARDAs work under his direction. Senator Blunt surprised Dr. Bright by giving him his personal cell phone number and directing him to call him if he ever wanted to discuss diagnostics, efforts to fight COVID-19, or anything that BARDA needed.
About two hours later, Dr. Kadlec and Mr. Shuy called Dr. Bright. They told him that his presentation to Senator Blunt must have been phenomenal. In describing his impression of the briefing, Dr. Kadlec asked Dr. Bright if he was familiar with the phrase catastrophic success. Dr. Kadlec then told Dr. Bright that he had good news and other news. Dr. Kadlecs good news was that Congress apparently had so much confidence in Dr. Bright that it was planning to give BARDA billions of dollars of additional funding, possibly in excess of $2 billion just to focus on diagnostics. According to Dr. Kadlec, Congress strongly believed in Dr. Bright and his ability to lead BARDA in combating COVID-19. Dr. Kadlec and Mr. Shuy were both extremely congratulatory, reiterating that Dr. Bright must have had a fantastic briefing with Senator Blunt.
Then, in order to create a pretext for Dr. Brights removal as BARDA Director, Dr. Kadlec fabricated a false narrative. Dr. Kadlec presented what he called his other news. He told Dr. Bright that Congress wanted BARDA and NIH to use the additional funding to work together on a special project focusing on diagnostics. Dr. Kadlec and Mr. Shuy then both disparaged NIH Director Francis Collins, calling him profane names and lamenting that Dr. Bright would have to find a way to collaborate with him on this project. According to Dr. Kadlec, Dr. Collins was trying to make political moves to take over some of BARDAs territory and assume primary responsibility for vaccine development. Dr. Kadlec instructed Dr. Bright that he was to get the money and write the checks while controlling Dr. Collins. Before ending the call, Dr. Kadlec told Dr. Bright that this additional funding was going to make Dr. Bright famous. Dr. Bright found the comments and friendly attitude confounding, particularly given Dr. Kadlecs hostile behavior towards him for months, if not years, as they repeatedly clashed on important issues.
— Footnotes —
30. Sarah Owermohle, FDA Official Steps into Vaccine Vacuum after Shakeup, POLITICO (Apr. 29, 2020), available at https://www.politico.com/news/2020/04/29/fda-official-coronavirus-vaccine-220858.
— End of Footenotes —
That evening, Dr. Collins emailed Dr. Bright: Id like the chance to talk with you about closer collaboration between NIH and BARDA on COVID-19. See email from F. Collins to R. Bright (Apr. 17, 2020), attached hereto as Exhibit 61. They made plans to talk in the morning and Dr. Bright worked through the night to prepare for the call. Believing that BARDA and NIH would be collaborating to develop diagnostics at the direction of Congress, Dr. Bright wanted to be prepared to discuss a high-level plan so that they could get started as soon as possible on this special project. That night, Dr. Bright called industry colleagues to discuss the issue and he outlined a strategy. The next morning, Dr. Bright called Dr. Kadlec to discuss the ideas he was planning to propose to Dr. Collins. Dr. Kadlec told Dr. Bright that his ideas were brilliant.
Unfortunately, Dr. Brights call with Dr. Collins did not go as planned. Dr. Collins began the call by telling Dr. Bright that he was going to become one of Dr. Collinss deputies at NIH, and then began berating him. He said something to the effect of, Were going to be working closely, and I just want to be clear with you about a few things. He then proceeded to tell Dr. Bright that Dr. Kadlec, Secretary Azar, and Congress all hated him, so according to Dr. Collins, he was doing Dr. Bright a favor by letting him come to NIH. Dr. Bright responded that he had just recently received a call from Dr. Kadlec saying Congress had such confidence in him and his organization that it was going to give BARDA billions of additional dollars. Dr. Bright concluded, So your comments confuse me, but I probably need to take this back to my boss to talk about it.
Dr. Bright then suggested that he and Dr. Collins discuss how to develop diagnostics to test people for COVID-19 and get Americans back to work. Dr. Bright shared his ideas, and Dr. Collins reacted positively. He said something to the effect of, That sounds good, but I dont understand why you dont think youre going to report to me like your boss said. Dr. Bright said he would talk to Dr. Kadlec to clarify his role. After the call, Dr. Bright immediately called Dr. Kadlec and relayed what Dr. Collins said. Dr. Kadlec responded by calling Dr. Collins a jackass and insisting that he was full of shit. He said that Dr. Bright would get the money from Congress and would run the show. The call concluded with Dr. Kadlecs assurances that he would take care of the confusion about Dr. Brights reporting structure.
Later that day, Dr. Bright received a frantic call from his Special Assistant, Greta Blattner. She told Dr. Bright that the BARDA communications team had just informed her that they had taken Dr. Brights name and image off the ASPR website. According to the communications team, Dr. Bright had accepted a new job at NIH. Dr. Bright called Dr. Kadlec, but he did not answer. Dr. Bright sent him a text message saying that he was removed from the website because someone said he was moving to NIH. Dr. Kadlec responded in one word, all capitalized: WHAT? He said nothing else, and he did not return Dr. Brights call. About 10:00 p.m. that night, Dr. Bright received a call from ASPR Director of Communications Gretchen Michael who congratulated Dr. Bright for being an ASPR employee again. She told him that she had been instructed to restore Dr. Brights name and image to the website. In an effort to determine who had given the directions to remove, then restore Dr. Bright to ASPRs website, Ms. Blattner made some phone calls at Dr. Brights direction. She soon learned that both directives came from Nikki Bratcher-Bowman, ASPR Director of Executive Management, who works for and reports only to Dr. Kadlec.
On Sunday, April 19, 2020, Dr. Bright conducted BARDA business as usual. While Dr. Collins told Dr. Bright that he was to report to him, Dr. Bright genuinely believed that Dr. Collins must have been mistaken. Even Dr. Kadlec had indicated that Dr. Collins was mistaken. Dr. Bright had no desire to work at NIH, and neither Dr. Kadlec nor anyone else had asked Dr. Bright if he wanted to transfer to NIH. Dr. Bright believed the website snafu must have been a misunderstanding, as well, especially because it was corrected within a day. That evening, Dr. Collins requested a phone call with Dr. Bright and they agreed to a call at 10:00 am the following morning.
Dr. Collins emailed Dr. Bright Monday morning before their call noting, I dont think were starting off on the right foot. He told Dr. Bright that he had spoken to Dr. Kadlec, and the two agreed that Dr. Bright was to be a senior advisor to Dr. Collins at NIH, and no longer an employee at BARDA. He further explained that Dr. Disbrow would become BARDAs Acting Director. Dr. Bright was stunned, and called Dr. Kadlec to relay what Dr. Collins had said in his email. Dr. Kadlec reiterated that Dr. Collins was a jackass. Dr. Bright asked if what Dr. Collins said was true, and Dr. Kadlec dodged the question and told Dr. Bright that he was going to have to work really closely with Dr. Collins. Dr. Bright asked if that meant he was being taken out of BARDA. Dr. Kadlec evaded again and said he would look into it. Immediately after this call, between 9:30 and 10:00 am that morning, Dr. Bright discovered that his email had been cut off.
Dr. Bright was late to his 10:00 am call with Dr. Collins. He told Dr. Collins that his email had been cut off and he was unable to access the videoconference portal, but he called in using a phone number that his Special Assistant was able to access from her email. Dr. Bright then explained that he was not trying to be difficult, but he remained confused because what Dr. Collins wrote in his email did not align with what Dr. Kadlec had just told him. Dr. Collins replied that he had talked that morning to Dr. Kadlec and the HHS Deputy Chief of Staff for Policy Paul Mango, who implements Secretary Azars policy, and both had communicated that the plan was for Dr. Bright to transfer to NIH. Dr. Collins then said something to the effect of: I believe youre being victimized here, youre caught in the crosshairs. I didnt see the need to move you out either. At Dr. Collinss suggestion, they ended the call so they could clear up any misunderstanding.
Shortly thereafter, Dr. Bright received a text message from Dr. Kadlec: Ive confirmed youve been assigned to NIH. Dr. Bright immediately called Dr. Kadlec, but once again he did not answer. Throughout the rest of the day. Dr. Bright repeatedly called both Dr. Kadlec and, in an attempt to reach Dr. Kadlec, Ms. Bratcher-Bowman. Neither of them answered his calls. Later that day, Dr. Bright read media reports that he had been transferred to a more limited position at NIH. On April 21, 2020, HHS released a statement to the media confirming Dr. Brights ouster as Director of BARDA. HHSs initial message was that Dr. Brights transfer from BARDA was part of a bold plan to accelerate the development and deployment of novel point-of-care testing platforms.(31) HHS also said that Dr. Bright would be tapped to lead a new shark tank effort to develop a COVID-19 test.(32)
On April 22, 2020, Dr. Bright and his counsel released a statement objecting to his removal as Deputy Assistant Secretary for Preparedness and Response and Director of BARDA and his involuntary transfer to a more limited and less impactful position at NIH. He stated: I believe this transfer was in response to my insistence that the government invest the billions of dollars allocated by Congress to address the COVID-19 pandemic into safe and scientifically vetted solutions, and not in drugs, vaccines and other technologies that lack scientific merit. I am speaking out because to combat this deadly virus, science not politics or cronyism has to lead the way. Dr. Bright stated that he intended to file a whistleblower complaint with the Office of Special Counsel.
In response, HHS Leadership engaged in a baseless smear campaign against Dr. Bright, asserting, for the first time, that Dr. Bright was removed from his position for poor performance. This rationale is baseless and is undercut entirely by the stellar performance appraisals Dr. Bright was given by Dr. Kadlec. Dr. Bright had also recently received a significant monetary performance bonus in December and was appointed the MCM Czar by Dr. Kadlec when the COVID-19 response was shifted from HHS leadership to FEMA in March. This claim also defies the confidence shown in Dr. Bright and his leadership of BARDA as evidenced by Congress appropriating $3.5 billion directly to BARDA for the COVID-19 response. In another blatant act of retaliation, NIH Director Francis Collins announced on April 29, 2020, that Dr. Bright would not lead the new shark tank effort to develop a COVID-19 test and that his precise role is under development. Dr. Bright has not been assigned any responsibilities and duties and remains in limbo. As of April 20, 2020, he stopped receiving a paycheck.
IV. HHSs involuntary transfer of Dr. Right violated the Whistleblower Protection Act.
The Whistleblower Protection Act of 1989 (WPA), protects federal employees who disclose evidence of illegal or improper government activities. Under the WPA, an agency may not take or threaten to take certain personnel actions because of a protected disclosure by an employee. An employee engages in a protected disclosure when he makes a formal or informal communication of information that he reasonably believes evidences any violation of any law, rule, or regulation or gross mismanagement, a gross waste of funds, an abuse of authority, or a substantial and specific danger to public health and safety. 5 U.S.C. 2302(b)(8)(A); Pub. L. No. 112-199, sec. 110, 126 Stat. 1465 (Nov. 27, 2012) (protecting disclosures that an employee reasonably believes are evidence of censorship related to research, analysis, or technical information that the employee believes is, or will cause, either a violation of law, rule or regulation or gross mismanagement, a gross waste of funds, an abuse of authority, or a substantial and specific danger to public health or safety). Protected disclosures include those made to a supervisor or to a person who participated in the activity that was the subject of the disclosure, as well as those made during the normal course of duties of an employee. Day v. Dept of Homeland Sec., 119 M.S.P.R. 589, 599 (2013).
— Footnotes —
31. Nathaniel Weixel, Director of Agency Behind Vaccine Development Leaves Role, THE HILL (Apr. 21, 2020), https://www.theinternetpatrol.com/brick-wall/ coronavirus-vaccine-development-departs.
32. Jeremy Diamond, Bright’s Ouster Shines Light on Months of HHS Turmoil, CNN (Apr. 23, 2020), available at https://www.theinternetpatrol.com/brick-wall/ coronavirus/index.html.
— End of Footnotes —
A. Dr. Bright made protected disclosures under the Whistleblower Protection Act.
Dr. Bright has engaged in numerous instances of protected activity under the WPA. First, in objecting to pressure from HHS leadership to ignore scientific merit and expert recommendations and instead to award lucrative contracts based on political connections and cronyism (as he did with the Aeolus, Alvogen, and Partner Therapeutics contracts), Dr. Bright conveyed information he reasonably believed evidenced an abuse of authority or gross mismanagement. As such, these communications were protected disclosures under 5 U.S.C. 2302(b)(8)(A)(ii); see also Embree v. Dept of Treasury, 70 M.S.P.R. 79, 85 (1996) (agency officials preferential treatment of specific company, to the detriment of agencys goals, is abuse of discretion); White v. Dept of the Air Force, 63 M.S.P.R. 90, 95 (1994) (characterizing gross mismanagement as management action or inaction which creates a substantial risk of significant adverse impact upon the agencys ability to accomplish its mission).
Indeed, Dr. Bright was so concerned about the improper role Mr. Clerici and a former employee turned consultant played in promoting a particular drug and their improper influence with Dr. Kadlec and HHS leaders that he requested the HHS Office of General Counsel initiate a procurement integrity violation investigation. This was a protected disclosure of a violation of law, rule, or regulation by Dr. Bright. 5 U.S.C. 2302(b)(8)(A)(i); see also Johnston v. Merit Sys. Prot. Bd., 518 F.3d 905, 910 (Fed. Cir. 2008) (employees disclosures to agency’s Office of Inspector General are protected under WPA); Reid v. Merit Sys. Prot. Bd., 508 F.3d 674, 677 (Fed. Cir. 2007) (internal complaints that agency action may violate Federal Acquisition Regulations is protected activity under WPA); Johns v. Dept of Veterans Affairs, 95 M.S.P.R. 106, 111 (2003) (internal complaints of improper contracting procedures are protected activity under WPA).
Dr. Bright also engaged in protected activity when he insisted that BARDA funds be apportioned in accordance with their expected benefit. As noted above, Dr. Bright objected to extending a contract that subject matter experts concluded had lost its value to the government (Aeolus), and he resisted the ASPRs efforts to fund drugs that subject matter experts concluded were inferior to other options (Oseltamivir), or which had not yet been properly tested (EIDD- 2801). By insisting BARDA allocate money to projects that aligned most closely with the mission of the agency to save lives and protect Americans, and refrain from funding projects unsupported by experts in the field, Dr. Bright made protected disclosures of a gross waste of funds. 5 U.S.C. 2302(b)(8)(A)(ii); see also Gilbert v. Dep’t of Commerce, 194 F.3d 1332 (Fed. Cir. 1999) ([E]ven if a particular expenditure is within the officials discretionary authority, a disclosure regarding that expenditure may qualify as a protected disclosure of a gross waste of funds . . . if a reasonable person would conclude that the expenditure is significantly out of proportion to the benefit reasonably expected to accrue to the government.).
Following the emergence of COVID-19, Dr. Bright engaged in protected activity when he implored HHS leadership to take urgent measures to prepare for the spread of this deadly virus. From January to March 2020, he repeatedly objected to the Administrations strategy of attempting to contain the virus outside of the United States; its failure to take action to devote resources to vaccine, drug, and diagnostic development; and its failure to secure and produce potentially promising drugs such as Remdesavir, and supplies such as respirators, masks, swabs and syringes. Dr. Brights advocacy for these appropriately aggressive measures constitutes protected disclosures of a substantial and specific danger to public health or safety under 5 U.S.C. 2302(b)(8)(A)(ii) because Dr. Bright reasonably believed that the information disclosed evidence[d] a danger . . . even if the alleged danger was created by a policy decision. Miller v. Dep’t of Homeland Sec., 111 M.S.P.R. 312, 31819 (2009) (employees criticisms protected under 5 U.S.C. 2302(b)(8) where the employee reasonably believed that the changes he identified in the agencys [procedures] constituted disclosure of substantial and specific dangers to public safety.); Johnston v. Merit Sys. Prot. Bd., 518 F.3d 905, 907 (Fed. Cir. 2008) (informing supervisor of concerns about public safety is protected under 2302(b)(8)).
When his calls for urgent action fell (sic) were dismissed and ignored, Dr. Bright sought political support outside of HHS. He met with White House Trade Advisor Peter Navarro in February 2020 to discuss actions necessary by HHS to combat COVID-19. His disclosures to Mr. Navarro about missteps by HHS were protected disclosures of gross mismanagement, and a substantial and specific danger to public health or safety. See McCarthy v. Intl Boundary & Water Comm: U.S. & Mexico, 116 M.S.P.R. 594, 615 (2011) (disclosure to White House about potential agency wrongdoing is protected under WPA). The following month, Dr. Bright disclosed to various members of Congressincluding Senator Steve Daines (R-MT), Senator Chris Coons (D-CT), Senator Roy Blunt (R-MO), Congresswoman Anna Eshoo (D-CA) and Congresswoman Rosa DeLauro (D-CT)that, among other things, HHS leadership delayed and withheld money from BARDA allocated by Congress, which hampered diagnostics, drug and vaccine development. These disclosures were protected under the WPA. See Chambers v. Dept of the Interior, 116 M.S.P.R. 17, 31 (2011) (statements to congressional staff members concerning practices that endangered the public constituted protected disclosures under the WPA); Parikh v. Dep’t of Veterans Affairs, 116 M.S.P.R. 197, 21314 (2011) (employees communication to senators about his concern for patient health and safety are protected disclosures under WPA).
Dr. Bright additionally engaged in protected activity when he resisted efforts to fall into line with the Administrations directive to promote the broad use of chloroquine and hydroxychloroquine, even though these drugs lacked scientific merit and had not received prior scientific vetting. In March 2020, scientific experts within BARDA and across HHS through the MCM TF concluded that data to date had shown no clinical benefit of chloroquine and hydroxychloroquine, and that there were scientific liabilities associated with Bayers donation of chloroquine tablets that came from foreign manufacturers that were not approved by the FDA. When Dr. Kadlec and others in the Administration spoke of flood[ing] New York and New Jersey with these drugs, Dr. Bright and his staff repeatedly voiced their concerns. Nevertheless, HHS publicly announced its acceptance of Bayers donation, and lauded chloroquine and hydroxychloroquine as potential therapeutics for COVID-19.(33) The HHS press release claimed that both drugs have shown activity in laboratory studies against coronaviruses, and [a]necdotal reports suggest that these drugs may offer some benefit in the treatment of hospitalized COVID- 19 patients. By making public disclosures contrary to the conclusions of its experts, and by failing to disclose the known risks of unapproved foreign drugs, HHS muzzled its experts and instead published information that was politically expedient. When Dr. Bright objected to HHS leaderships censorship of expert opinion in favor of a political win, he engaged in protected activity under the WPA. See Pub. L. No. 112-199, sec. 110, 126 Stat. 1465 (Nov. 27, 2012) (protecting disclosures that an employee reasonably believes is evidence of censorship related to research, analysis, or technical information that the employee reasonably believes is, or will cause …gross mismanagement, a gross waste of funds, an abuse of authority, or a substantial and specific danger to public health or safety).
Finally, Dr. Bright engaged in protected activity when concerned that his objections were not getting any traction within HHS and lives were at stake he confirmed to a reporter that HHS had accepted a donation of drugs from Pakistan and India that had not been approved by the FDA and were potentially toxic. Dr. Bright was concerned that HHS actions would seriously harm, or even kill, members of the American public. He agreed to speak with a reporter and confirm this information about the dangers of chloroquine, which was neither classified nor confidential, because he believed transparency on this issue would save lives. The disclosed danger was sufficiently substantial and specific to warrant protection under the WPA because it identified an objectively significant and serious danger to public health and safety namely, the mass consumption of unvetted and potentially toxic drugs. See Dept of Homeland Sec. v. MacLean, 574 U.S. 383, 395 (2015); Chambers v. Dept of the Interior, 116 M.S.P.R. 17, 2829 (2011) (employees emails to a Washington Post reporter were protected disclosures because she reasonably believed they disclosed a substantial and specific danger to public health or safety).
With each of these actions, Dr. Bright sought to advance public health and safety by advocating for measures that he and other subject matter experts concluded would best protect the American public. Dr. Bright certainly had a reasonable belief that his disclosures were protected because a disinterested observer with knowledge of the essential facts . . . could reasonably conclude that overriding the recommendations of public health experts poses a substantial and specific danger to public health. Bradley v. Dep’t of Homeland Sec., 2016 WL 4586169 (M.S.P.B. Sept. 1, 2016) (citing 5 U.S.C. 2302(b)(8)). See also Special Counsel ex rel. Cameron v. Dept of Veterans Affairs, 2018 WL 6267107, at *2 (M.S.P.B. Nov. 30, 2018) (VA doctors disclosures protected under 5 U.S.C. 2302(b)(8) when he emailed Chief of Anesthesiology, his supervisor, and his supervisors deputy to oppose a hospital policy because it placed patients at risk); Johnston v. Merit Syst. Prot. Bd., 518 F.3d 905, 909 (Fed. Cir. 2008) (objection to nuclear weapons transportation policy change to involve less educated and experienced personnel was a protected disclosure regarding public safety).
— Footnotes —
33. Press Release, HHS, HHS accepts donations of medicine to Strategic National Stockpile as possible treatments for COVID-19 patients (Mar. 29, 2020), available at https://www.theinternetpatrol.com/brick-wall/ stockpile-as-possible-treatments-for-covid-19-patients.html.
— End of Footnotes —
B. HHS took a personnel action against Dr. Bright.
HHSs sudden, involuntary removal of Dr. Bright from his position as BARDA Director in the midst of the COVID-19 pandemic was a prohibited personnel action. Under the WPA, personnel actions include a transfer, reassignment, and any significant change in duties, responsibilities, or working conditions. 5 U.S.C. 2302(a)(2)(A). The definition of personnel action must be interpreted broadly. Singleton v. Ohio Nat. Guard, 77 M.S.P.R. 583, 587 (1998). When HHS removed Dr. Bright from his position as BARDA director and assigned him to work at the NIH, it engaged in a prohibited personnel practice. See Onasch v. Dept of Transp., No, 1994 WL 283861 (M.S.P.B. June 17, 1994) (reassignment, combined with loss of responsibility and the significant reduction in the number of persons supervised, is prohibited personnel action under WPA); Johns v. Dep’t of Veterans Affairs, No. CH-1221-98-0525-B-1, 2003 WL 22570157
(M.S.P.B. Aug. 14, 2003) (changes to whistleblowers duties and resources may constitute significant change in duties, responsibilities, or working conditions).
C. Dr. Brights protected disclosures were a contributing factor in the agencys personnel action.
Dr. Bright will be able to demonstrate that his protected disclosures were a contributing factor in the agencys personnel action because of Dr. Kadlec and Secretary Azars awareness of his whistleblowing activity, and the timing of the adverse action. Johnston v. Merit Sys. Prot. Bd., 518 F.3d 905, 912 (Fed. Cir. 2008) ( [A] whistleblower need only allege that the deciding official knew of the disclosure and that the adverse action was initiated within a reasonable time of that disclosure in order to make a prima facie case that the disclosure was a contributing factor in the adverse action.) (citing 5 U.S.C. 1221(e)(1)). See also Redschlag v. Dept of Army, 89 M.S.P.R. 589, 635 (2001) (disclosures were contributing factor in whistleblowers removal when they were made approximately 21 months, and then slightly over a year, before the agency removed her).
For years, Dr. Kadlec was frustrated by Dr. Brights efforts to undermine his agenda to award contracts based on political and personal connections. Dr. Bright resisted Dr. Kadlecs pressure to award contracts that were contrary to the recommendations of subject matter experts, and Dr. Kadlec was increasingly dismissive of and hostile to Dr. Brights objections. Dr. Kadlecs displays of frustration towards Dr. Brights protected disclosures are evidence that Dr. Brights protected activity was a contributing factor in his ultimate removal. See Whitmore v. Dep’t of Labor, 680 F.3d 1353, 1376 (Fed. Cir. 2012) (fact that whistleblowers disclosures marked the beginning of his increasingly strained relationships with agency officials is evidence of causation); Fellhoelter v. Dep’t of Agric., 568 F.3d 965, 971 (Fed. Cir. 2009) ([E]vidence of an employee’s assertions of misconduct by a supervisor can be relevant to whether the employee has made a protected disclosure and also whether the supervisor has a strong motivation to retaliate.); Kinan v. Dep’t of Def., 87 M.S.P.R. 561, 569 (2001) (finding requisite causation where supervisor displayed frustration by employees whistleblowing).
After the emergence of COVID-19, Dr. Bright angered HHS leadership when he implored them to take urgent measures to prepare for the spread of this deadly virus. After the first HHS COVID-19 meeting on January 23, 2020, Mr. Shuy told Dr. Bright that he had caused a shit storm by requesting additional money for BARDA in front of Secretary Azar. See Ayers v. Dep’t of Army, 123 M.S.P.R. 11, 24 (M.S.P.B. Nov. 2, 2015) (finding causation in part because of agencys hostile reaction to whistleblower disclosures). Similarly, in the second HHS COVID- 19 meeting that Dr. Bright attended on January 27, he pushed for obtaining virus samples from other countries in order to quickly proceed on vaccine development, and was chastised for raising the issue by Dr. Nancy Messonnier from the CDC, and by the Deputy Secretary of HHS, Eric Hargan. On this occasion, he was accused of causing a commotion by HHS Chief of Staff Brian Harrison. Tellingly, neither Dr. Bright nor anyone from BARDA was invited back to any future COVID-19 meetings after he had caused a shit storm and a commotion by raising these legitimate issues. See Mattil v. Dept of State, 118 M.S.P.R. 662, 671 (2012) (excluding the [whistleblower] from communications related to ongoing events in which he was involved is evidence of retaliation).
Over the next two months, as the country continued to reel from the worsening pandemic and the death count mounted each day, Congress and the White House became more interested in the work of HHS and BARDA in combatting the virus. Dr. Bright was contacted by members of Congress and White House staff to discuss the issue. Secretary Azar and Dr. Kadlec were particularly angered by Dr. Brights meetings with Mr. Navarro at the White House, which exposed HHSs lack of urgency and focus on addressing the pandemic. Dr. Brights meetings with Mr. Navarro helped propel the White House Task Force to issue policy directive for HHS. Dr. Kadlec responded negatively to Dr. Brights meetings with Mr. Navarro. As an initial matter, he withheld approval for Dr. Bright to meet with Mr. Navarro until Mr. Navarro personally called his office. After Dr. Bright and Mr. Navarros first meeting, Dr. Kadlec emailed employees in Secretary Azars office with the derisive subject line, Weekend at Peters conspiring with them to keep tabs on communication between Dr. Bright and Mr. Navarro, suggesting that senior staff within the Secretarys office get a back brief from Rick Bright on his time with Navarro. See Exhibit 23. This provides additional evidence of Dr. Kadlecs, as well as the Secretary Azars, displeasure with these protected disclosures. See Special Counsel ex rel. Alicea v. Dept of Def., 2016 WL 7448347 (M.S.P.B. Dec. 23, 2016) (finding causation in part because, after protected disclosures, supervisor showed hostility and began to more closely monitor whistleblower).
Similarly, Dr. Kadlec reacted negatively to Dr. Brights meetings with members of Congress, and the subsequent direct appropriation by Congress to BARDA. The CARES Act, which appropriated $3.5 billion directly to BARDA, made it harder for the Secretary and ASPR to withhold, siphon off, or otherwise control BARDAs funds. When Dr. Kadlec learned of the possibility of a direct appropriation to BARDA, he emailed Dr. Bright demanding to know if Dr. Bright was requesting that Congress fund BARDA over ASPR?! See Exhibit 46. When Dr. Bright responded that members of Congress had been reaching out to him to discuss funding, Dr. Kadlec responded that Mr. Shuy needed to review all of BARDAs submissions to Congress. Mr. Shuy subsequently instructed Dr. Bright to not reach back out to congressional offices. Id. Dr. Kadlecs negative reaction to Dr. Brights communications with members of Congress less than a month before his reassignment is further evidence that Dr. Brights protected communications were a contributing factor in his removal. See Special Counsel ex rel. Cameron v. Dept of Veterans Affairs, 2018 WL 6267107, at *3 (M.S.P.B. Nov. 30, 2018) (finding requisite causation in part because supervisors displayed hostility towards whistleblower as a result of his disclosures): Kinan v. Dep’t of Def., 87 M.S.P.R. 561, 569 (2001) (finding requisite causation where agency had motive to retaliate, and supervisor displayed frustration by employees whistleblowing). Following Dr. Brights protected disclosure to the journalist about HHSs political motivation for making chloroquine and hydroxychloroquine widely availablethat the White House wanted to flood New York and New Jersey with the drug Mr. Shuys warning that Dr. Bright should be careful is tantamount to direct evidence of retaliatory motive. See Corriveau v. Dept of Navy, 2015 WL 5210185 (M.S.P.B. Sept. 4, 2015) (statements that employees may face repercussions for protected disclosures may provide direct evidence of retaliatory motive).
D. HHS would not have transferred Dr. Bright to NIH in the absence of his protected disclosures.
Any attempt by HHS to argue that it would have transferred Dr. Bright to NIH in the absence of his protected disclosures will fail. See Whitmore v. Dep’t of Labor, 680 F.3d 1353, 1372 (Fed. Cir. 2012) (proving that an agency would have removed an employee regardless of his whistleblowing is a high burden). First, the evidence in support of the reasons HHS provided for transferring Dr. Bright to NIH are extremely weak and have been shifting and conflicting. The agency has to date made no efforts to involve Dr. Bright in the bold plan to accelerate the development and deployment of novel point-of-care testing platforms that it initially claimed was the basis for Dr. Brights involuntary transfer. The absence of any evidence that HHS is in fact carrying out such a plan fatally undermines this explanation for Dr. Brights transfer. See Rumsey v. Dept of Justice, 120 M.S.P.R. 259, 275 (2013) (lack of contemporaneous documentation of agencys justification for personnel action supported finding of retaliation, even though deciding official testified consistently with justification). Logically, it makes no sense that HHS would appoint Dr. Bright to carry out a plan to increase the nations coronavirus testing capacity in the midst of a global pandemic without at least apprising him of that plan.
HHS has since claimed that it transferred Dr. Bright to NIH because Dr. Bright mismanaged his office and mistreated his staff. Not only are the agencys shifting explanations for Dr. Brights involuntary transfer further evidence of retaliation, cf. Geleta v. Gray, 645 F.3d 408, 413 (D.C. Cir. 2011) (shifting and inconsistent justifications for adverse action are probative of pretext under Title VII), but Dr. Brights most recent performance review and long list of accomplishments as Director of BARDA demonstrate his strong performance and effectiveness as a leader in this position. In Dr. Brights most recent performance review, from September 2019, Dr. Kadlec praised both the quality and speed of BARDAs work under Dr. Bright’s leadership, noting that BARDA continues to develop and licensure (sic) of medical countermeasures at a rate that is well above the industry average and certainly a subject of their envy. Dr. Kadlec awarded Dr. Bright the highest performance rating of 5 in all but one category, Leading People, in which he received a 4.(34) But Dr. Kadlec nevertheless praised Dr. Bright for leading his staff effectively and made no criticisms of his management style.
BARDAs many successes under Dr. Brights leadership, and especially during the ongoing COVID-19 health crisis, belie any suggestion that he mismanaged his office. At the beginning of his tenure, Dr. Bright confronted the U.S. Zika outbreak by prioritizing the development of diagnostic tests, increasing testing capacity nationwide and eventually shepherding the first commercially-available diagnostic test to FDA approval. He also doubled down on BARDAs efforts to combat the Ebola virus, prioritizing vaccine development and providing a consistent stream of funding to private partners even after the WHO declared an end to the public health emergency of international concern in West Africa. This resulted in a historical success: the worlds first FDA-approved Ebola vaccine. When COVID-19 emerged as a global threat, Dr. Bright worked tirelessly to secure the U.S. mask supply in face of opposition from Dr. Kadlec and others at HHS and within a matter of days secured a military air bridge to transport testing swabs from Italy to the U.S. Finally, in the month prior to his removal, Dr. Bright secured the first-ever Congressional appropriation directly to BARDA after meeting directly with members of Congress and explaining to them how BARDA used its funds to support COVID-19 treatments, diagnostics, and vaccinesa clear indication of the lawmakers confidence in his work and leadership.
— Footnotes —
34. A rating of 5 demonstrates exceptional performance. A rating of 4 demonstrates a very high level of performance.
— End of Footnotes —
In addition to impugning Dr. Brights job performance as Director of BARDA, HHS has also claimed that Dr. Bright abused his authority by taking unilateral action to award a $456 million contract to Janssen, a subsidiary of Johnson & Johnson, to develop a COVID-19 vaccine. This is demonstrably false. As discussed above, following Dr. Brights initial contact with Janssen Chief Scientific Officer Dr. Paul Stoffels, Janssen submitted a formal proposal that was reviewed and recommended for approval by BARDA subject matter experts. After consulting with Dr. Bright, and on the recommendation of BARDAs subject matter experts, Dr. Disbrow submitted a request for funding directly to Dr. Kadlec. Dr. Kadlec himself approved the request that same day. Dr. Bright therefore did take any inappropriate unilateral action with respect to the Johnson & Johnson contract, and this explanation for his involuntary transfer to NIH is false. See Whitmore v. Dept of Labor, 680 F.3d 1353, 1369 (Fed. Cir. 2012) (veracity and reliability of agencys evidence alleged explanation of personnel action is relevant to assess independent causation).
Second, HHS officials had a strong motives for retaliating against Dr. Bright: concealing the agencys failure to act on Dr. Brights early warnings about the novel coronavirus. Smith v. Gen. Servs. Admin., 930 F.3d 1359, 1366 (Fed. Cir. 2019) (agency had motive for retaliating against employee where it failed to address employees repeated disclosures about agencys mismanagement). The agencys desire to preserve the Administrations narrative about drugs like chloroquine and hydroxychloroquine, the safety and efficacy of which Dr. Bright repeatedly called into question, provided additional motivation to transfer him away from BARDA. Dr. Brights persistent refusal to award contracts for political reasons instead of on the basis of scientific merit, meetings with Congress and Mr. Navarro over Dr. Kadlecs objections, and pushback against the Administrations efforts to make chloroquine and hydroxychloroquine widely available despite their health and safety risks all provide additional motive for HHS to retaliate against him The agencys subsequent efforts to smear Dr. Bright by telling media outlets that he hampered BARDAs effectiveness during the coronavirus outbreak only underscore its retaliatory motive for his removal. Additionally, the close temporal proximity between Dr. Brights protected disclosures, which occurred as recently as April 17, 2020, and his involuntary transfer on April 21, 2020, constitutes still more evidence of retaliatory motive. See Aquino v. Dep’t of Homeland Sec., 121 M.S.P.R. 35, 49 (2014) (temporal proximity of six days between employees protected disclosure and personnel action suggests a strong retaliatory motive).
Taken together, these facts demonstrate that HHS would not have transferred Dr. Bright to NIH in the absence of his protected disclosures.
E. As a result of HHSs illegal retaliation, the OSC should request HHS to stay its transfer of Dr. Bright.
Because there are reasonable grounds to believe that a prohibited personnel practice occurred, the OSC should request that HHS stay the personnel action and reinstate Dr. Bright as BARDA Director. See 5 U.S.C. 1214(b)(1)(A)(i). An initial stay is designed to permit OSC to complete its investigation and may be granted on the basis of relatively little information. Special Counsel v. U.S. Fish & Wildlife Serv., Dep’t of Interior, 62 M.S.P.R. 388, 392 (1994).
Typically, if HHS does not informally agree to a stay, the OSC could request that any member of the Merit Systems Protection Board (MSPB) order a stay while the OSC completes its investigation. A stay request shall be granted, unless the [Board] member determines that, under the facts and circumstances involved, such a stay would not be appropriate. 5 U.S.C. 1214(b)(1)(A)(ii). The Board will view the record in the light most favorable to the Special Counsel and will grant the stay request so long as it falls within the range of rationality. Special Counsel ex rel. Cefalu v. Dept of Justice, 2012 WL 11893480, at *1 (M.S.P.B. Oct. 23, 2012).
Currently, however, there are no members of the MSPB. President Trump has nominated three people to fill the three open positions Dennis Dean Kirk (nominated March 8, 2018), Julia Akins Clark (nominated June 20, 2018), and B. Chad Bungard (nominated April 25, 2019) but to date, the Senate has taken no action to confirm them. This lack of a Board quorum, indeed the lack of any Board members, makes it impossible for such a stay to be ordered by anyone other than the HHS Secretary. HHS violated the WPA by removing Dr. Bright from his position because he made protected disclosures in the best interest of the American public. Dr. Bright should not now be denied the right to have his complaint investigated fully and fairly before he is formally transferred to NIH a move that will harm not only him, but the country as well. Therefore, the OSC should request a stay, and the Secretary Azar should grant that stay.
—
Useful Acronyms
ASFR Assistant Secretary for Financial Resources
ASPR Assistant Secretary for Preparedness and Response
BAA Broad Agency Announcement
BARDA Biomedical Advanced Research and Development Authority CARES Coronavirus Aid, Relief, and Economic Security
CDC Centers for Disease Control and Prevention
CIP Critical Infrastructure Protection
CO Contract Officer
COR Contract Officer Representative
DHS Department of Homeland Security
DLG Disaster Leadership Group
DOD Department of Defense
DTRA Defense Threat Reduction Agency
EUA Emergency Use Authorization
FAR Federal Acquisition Regulation
FDA Food and Drug Administration
FEMA Federal Emergency Management Agency
FRMM Flu Risk Management Meeting
GAO Government Accountability Office
HCA Head of Contracting Activity
HHS Department of Health and Human Services
IG Inspector General
IGCE Independent Government Cost Estimate
IND Investigational New Drug
IPR In-Process Review
JOC Joint Oversight Committee
MCM Medical Countermeasure
MCM TF Medical Countermeasures Task Force
NCIRD National Center for Immunization and Recpitory Diseases
NIAID National Institute of Allergy and Infectious Diseases
NIH National Institute of Health
NIOSH National Institute of Occupational Safety and Health
OGC Office of General Counsel
OIG Office of Inspector General
OSC Office of Special Counsel
PHEMCE Public Health Emergency Medical Countermeasures Enterprise
PIA Procurement Integrity Act
PPE Personal Protective Equipment
RCT Randomized Controlled Trial
RFP Request for Proposals
SNS Strategic National Stockpile
SSA Source Selection Authority
TEP Technical Evaluationi Panel
USDA United States Department of Agriculture
VA Department of Veterans’ Affairs
VTM Viral Transport Media
WHO World Health Organization
WPA Whistleblower Protection Act
Useful Titles
Christopher Abbott – White House Senior Policy Advisor
Steven Adams – Acting Director of SNS (January 2020 to March 2020), Deputy Director of SNS (January 1999 to January 2020)
Jennifer Alton – Senior Consultant to Dr. Kadlec
Stacy Amin – Chief Counsel of FDA
Dr. Kimberly Armstrong – Chief of Therapeutics for Influenca and Emerging Infectious Diseases, BARDA
Alex Azar – Secretary of Health and Human Services
Joffrey Benford – Director of Contract Management and Acquisition, BARDA
Greta Blattner – Special Assistant to the Director, BARDA
Nikki Bratcher-Bowman – Director of Executive Management, ASPR
Dr. Rick Bright – Deputy Assistant Secretary for Preparedness and Response and Director of BARDA
Mike Bowen – Co-Owner and Executive Vice President, Prestige Ameritech
Greg Burel – Director of SNS (April 2007 to January 2020)
Dr. Michael Callahan – Consultant to Dr. Kadlec
Robert Charrow – General Counsel of HHS
John Clerici – Pharmaceutical industry consultant
Dr. Francis Collins – Director of NIH
Kevin Cooper – Acting Director of SNS (March 2020 to present)
Dr. Gary Disbrow – Deputy Assistant Secretary and Director of Medical Countermeasures Programs, BARDA
Dr. Ruben Donis – Deputy Director of Influenza and Emerging Infectious Diseases Division, BARDA
Katherine Eban – Investigative Journalist
Stanley Erck – Chief Executive Officer, Novavax
Schuyler Eldridge – Head of Contracting Activity, ASPR
Mark Esper – Secretary of Defense
Dr. Jessica Falcon – Deputy Assistant Secretary and Director, Office of Security, Intelligence, and Information Management, ASPR
Dr. Tremel Faison – Director of Regulatory and Quality Affairs, BARDA
Maj. Jeffrey Froude – Deputy Division Chief, DTRA
Peter Gaynor – Administrator of the Federal Emergency Management Agency
Adm. Brett Giroir – Assistant Secretary for Health, HHS
Dr. Ronald Hahn – Director of Chemical and Biological Technologies, DTRA
Dr. Stephen Hahn – Commissioner of Food and Drugs
Joseph Hamel – Strategic Innovation and Emerging Technology Manager, ASPR
Eric Hargan – Deputy Secretary, HHS
Brian Harrison – Chief of Staff, HHS
Dr. David (Chris) Hassell – Senior Science Advisor, ASPR
Dr. Christopher Houchens – Acting Director, Division of CBRN Medical Countermeasures, BARDA
Wendy Holman – Chief Executive Officer, Ridgeback Biotherapeutics LP
Dr. Mary Homer – Chief of Radiological and Nuclear Countermeasures, BARDA
Rosemary Humes – Deputy Director of Detection, Diagnostics and Devices Infrastructure Division, BARDA
Dr. Dan Jernigan – Director of the Influenza Division, NCIRD
Dr. Robert Johnson – Director of Influenza and Emerging Infectious Diseases Division, BARDA
Dr. Robert Kadlec – Assistant Secretary for Preparedness and Response
Dr. Larry Kerr – Director of Pandemics and Emerging Threats, Office of Global Affairs, HHS
Jared Kushner – Senior Advisor to the President
Dr. Linda Lambert – Deputy Assistant Secretary and Director of Medical Countermeasures Program Support Services, BARDA
Dr. Cliff Lane – Deputy Director for Clinical Research and Special Projects, NIAID
Judy Laney – Chief of Chemical Medical Countermeasures, BARDA
Dr. Joe Larsen – Acting Director, Division of CBRN Medical Countermeasures, BARDA (February 2017 to July 2018)
Paul Mango – Deputy Chief of Staff for Policy, HHS
Dr. Nancy Messonnier – Director of the National Center for Immunization and Respiratory Diseases
John McManus – Chief Executive Officer, Aeolus Pharmaceuticals
Christopher Meekins – Deputy Assistant Secretary and Chief of Staff, ASPR (July 2017 to January 2019)
Gretchen Michael – Director of Communications, ASPR
Joanna Miller – White House Policy Analyst, Office of Trade and Manufacturing Policy
Mick Mulvaney – Acting White House Chief of Staff (January 2019 to March 2020)
Peter Navarro – White House Trade Advisor, Office of Trade and Manufacturing Policy
Robert O’Brien – White House National Security Advisor
Dr. George Painter – Director, Emory Institute for Drug Development and President and Chief Executive Officer, Drug Innovation Ventures at Emory
Dr. Anita Patel – Senior Advisor for Pandemic Medical Care and Countermeasures, CDC
Jay Petillo – Director, Office of Financial Planning and Analysis, ASPR
Rear Adm. John Polowczyk – Vice Director for Logistics of the Joint Chiefs of Staff
Dr. Robert Redfield – Director of the Centers for Disease Control and Prevention
Dan Reese – President, Prestige Ameritech
Brian Rosen – Senior Vice President of Public Policy and Commercial Strategy, Novavax
Dr. Jeffrey Shuren – Director of the Center for Devices and Radiological Health, FDA
Bryan Shuy – Deputy Assistant Secretary and Chief of Staff, ASPR
Judy Stecker – Deputy Chief of Staff for Operations and Strategy, HHS
Dr. Kevin Tracey – Executive Vice President of Research, Northwell Health
Cicely Waters – Director of Office of External Affairs, ASPR
Dr. Laura Wolf – Director, Division of Critical Infrastructure Protection, ASPR
Dr. Janet Woodcock – Director, Center for Drug Evaluation and Research, FDA
Dr. Kevin Yeskey – Principal Deputy Assistant Secretary, ASPR
###
Link to PDF of Rick Bright Whistleblower Complaint Against DHHS
The Internet Patrol is completely free, and reader-supported. Your tips via CashApp, Venmo, or Paypal are appreciated! Receipts will come from ISIPP.
CashApp us
Venmo us
Paypal us






